
SLIDE 1
3/9/2019 1
PH treatment in Single Ventricule
Marilyne Lévy, Necker- Paris - France UCSF from 2016 to 2019
« Single » Ventricle BUT Multiple…
- Ventricular function: LV? RV?
- Atrial pressure : AV valve ?
- Pulmonary circulation ?
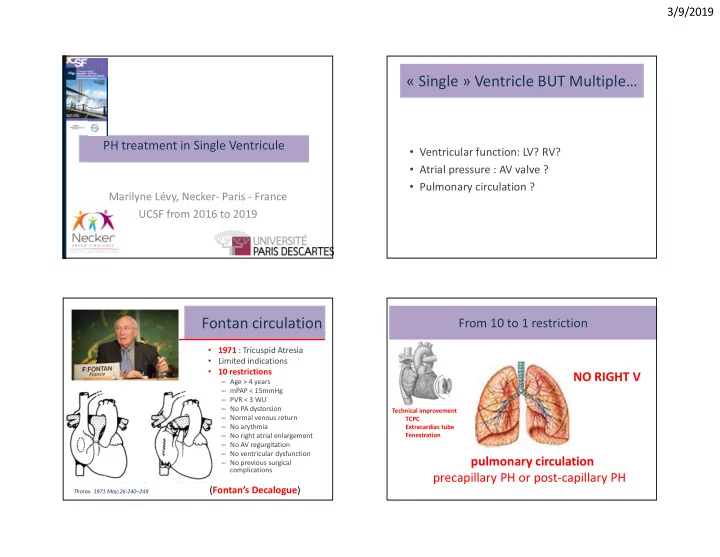
Fontan circulation
- 1971 : Tricuspid Atresia
- Limited indications
- 10 restrictions
– Age > 4 years – mPAP < 15mmHg – PVR < 3 WU – No PA dystorsion – Normal venous return – No arythmia – No right atrial enlargement – No AV regurgitation – No ventricular dysfunction – No previous surgical complications
- Thorax. 1971 May;26:240–248
(Fontan’s Decalogue)
From 10 to 1 restriction pulmonary circulation precapillary PH or post-capillary PH
Technical improvement TCPC Extracardiac tube Fenestration