SLIDE 11 11
Factors Contributing to Resistant Hypertension
(Sarafidis and Bakris, JACC 52(22): 1749-57)
Excess sodium intake Volume retention from kidney disease Inadequate diuretic therapy
Obesity Diabetes mellitus Older age
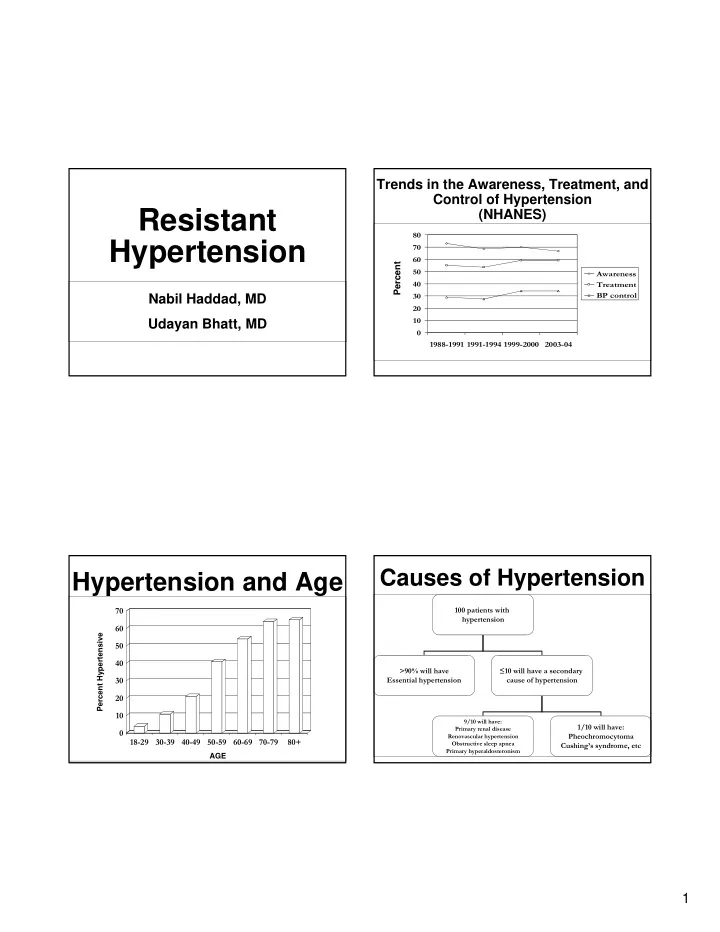
- Identifiable causes of hypertension
Renal parenchymal disease Renovascular disease Primary aldosteronism Obstructive sleep apnea Pheochromocytoma Cushing’s syndrome Thyroid diseases Aortic coarctation Intracranial tumors
When to look for secondary hypertension?
- Onset of hypertension before puberty or over
the age of 55
- Severe or difficult to treat hypertension
- A change in the ability to control blood pressure
- Hypertension in the absence of a family history
- A high index of suspicion based on knowing the way in
which various forms of secondary hypertension occur Symptoms - palpitations, sweating Signs - body habitus, bruits Laboratory evaluation – elevated Cr, hypokalemia
Treatment of Resistant Hypertension
- Exclusion of other causes of pseudo-resistance
- Treatment of a secondary etiology, when possible
- Identification and modification of factors
contributing to resistant hypertension
- Targeting different mechanisms of hypertension
(volume overload, Renin-Angiotension- Aldosterone system, vascular resistance)
Summary
- A minority of patients with hypertension have an
identifiable cause- known as secondary HTN
- Identification of the cause and its treatment has
potential to significantly improve BP control and sometimes, cure it
- Endocrine abnormalities are important in causing
secondary hypertension
- Renovascular disease is significantly more
common cause of HTN than understood