
SLIDE 1
1
Kate Frómeta, CNM Assistant Professor Department of Obstetrics and Gynecology UCSF
Re-examining Prenatal Care
Antepartum and Intrapartum Management Conference San Francisco, CA
No Disclosures Prenatal Care
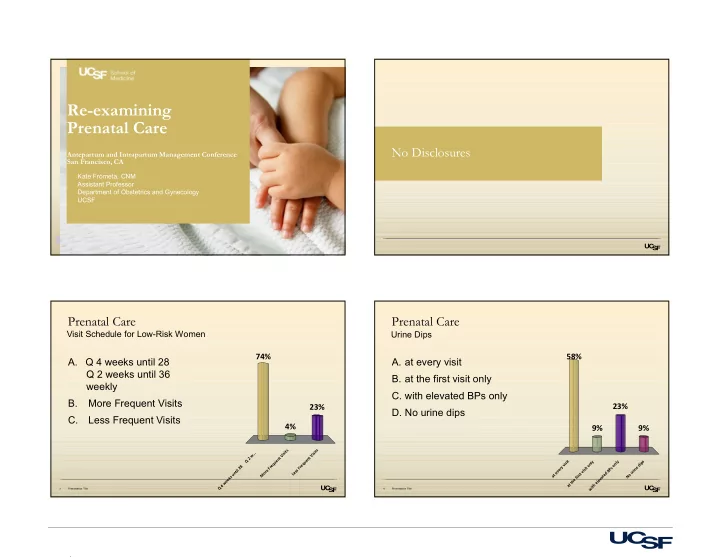
- A. Q 4 weeks until 28
Q 2 weeks until 36 weekly B. More Frequent Visits C. Less Frequent Visits
Presentation Title 3
Visit Schedule for Low-Risk Women
Q 4 w e e k s u n t i l 2 8 Q 2 w . . . M
- r
e F r e q u e n t V i s i t s L e s s F r e q u e n t V i s i t s
74% 23% 4%
Prenatal Care
- A. at every visit
- B. at the first visit only
- C. with elevated BPs only
- D. No urine dips
Presentation Title 4
Urine Dips
a t e v e r y v i s i t a t t h e f i r s t v i s i t
- n
l y w i t h e l e v a t e d B P s
- n
l y N
- u
r i n e d i p s