
SLIDE 1
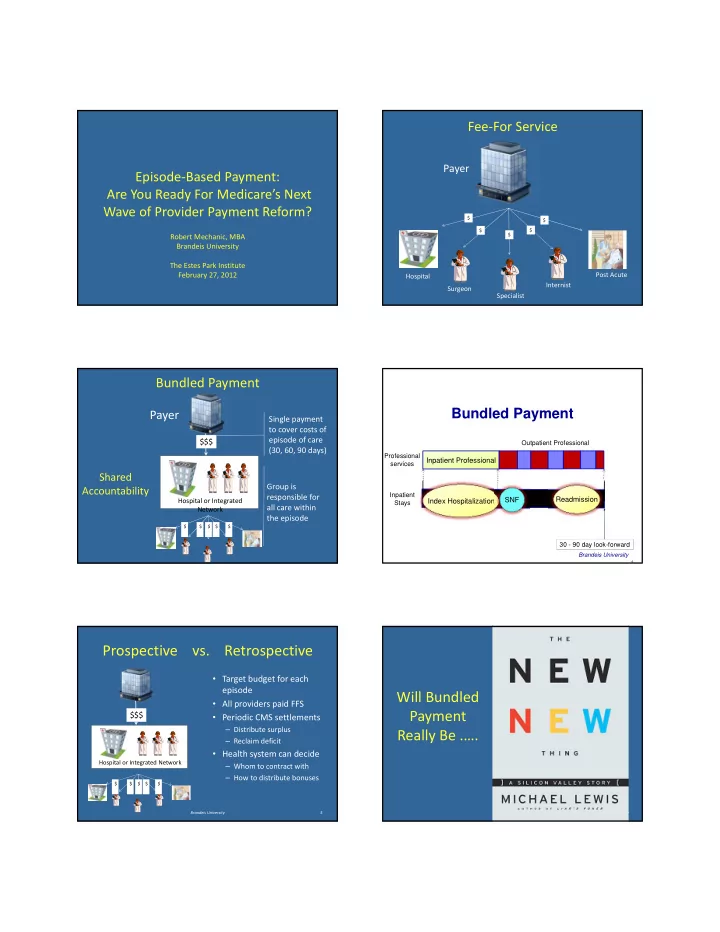
Episode‐Based Payment: Are You Ready For Medicare’s Next Wave of Provider Payment Reform?
Robert Mechanic, MBA Brandeis University The Estes Park Institute February 27, 2012
Fee‐For Service
Payer
Hospital Specialist Surgeon
$ $ $ $ $
Internist Post Acute
Bundled Payment
Hospital or Integrated Network
$$$ Single payment to cover costs of episode of care (30, 60, 90 days)
Payer
$ $ $ $ $
Group is responsible for all care within the episode
Shared Accountability
4
30 - 90 day look-forward
Index Hospitalization Inpatient Professional
Outpatient Professional Professional services Inpatient Stays
Brandeis University
Readmission SNF
Bundled Payment
Prospective vs. Retrospective
- Target budget for each
episode
- All providers paid FFS
- Periodic CMS settlements
– Distribute surplus – Reclaim deficit
- Health system can decide
– Whom to contract with – How to distribute bonuses
Brandeis University 5
Hospital or Integrated Network
$$$
$ $ $ $ $
Will Bundled Payment Really Be .….
Brandeis University
6