
SLIDE 1
4/15/2019 1
Pressure Injuries – Prevent, Treat and Sustain Gains
Joyce Black, PhD, RN, FAAN University of Nebraska Medical Center Omaha, NE
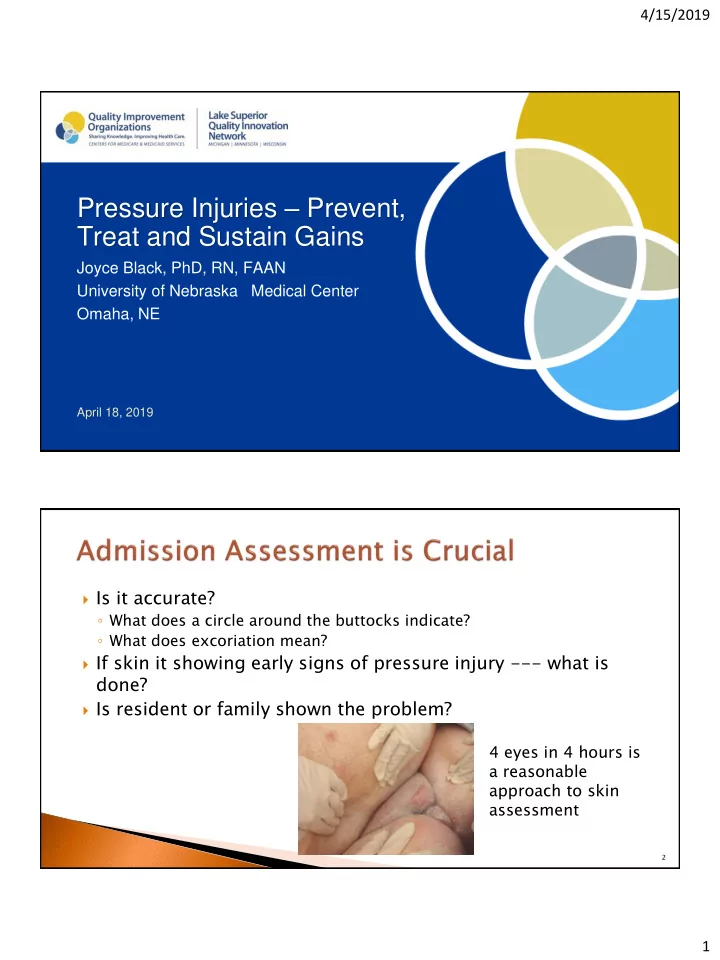
April 18, 2019 Is it accurate?
- What does a circle around the buttocks indicate?
- What does excoriation mean?
If skin it showing early signs of pressure injury --- what is
done?
Is resident or family shown the problem?
4 eyes in 4 hours is a reasonable approach to skin assessment
2