
SLIDE 1
Sarah Vest Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy AlSHP Fall Meeting September 30, 2016
Pharmacists:
Discuss the rationale for modifications to the sepsis definitions Describe the updated sepsis definitions (Sepsis‐3)
Technicians:
Define sepsis and septic shock
I have no actual or potential conflict of interest in relation to this program Need to differentiate sepsis from infection Improved understanding of sepsis pathophysiology
Previous definitions focused on SIRS criteria
Variable definitions – inconsistent reporting
Sepsis vs. severe sepsis Sepsis syndrome Septicemia
Singer M, et al. JAMA. 2016;315(8):801‐810. Singer M, et al. JAMA. 2016;315(8):801‐810.
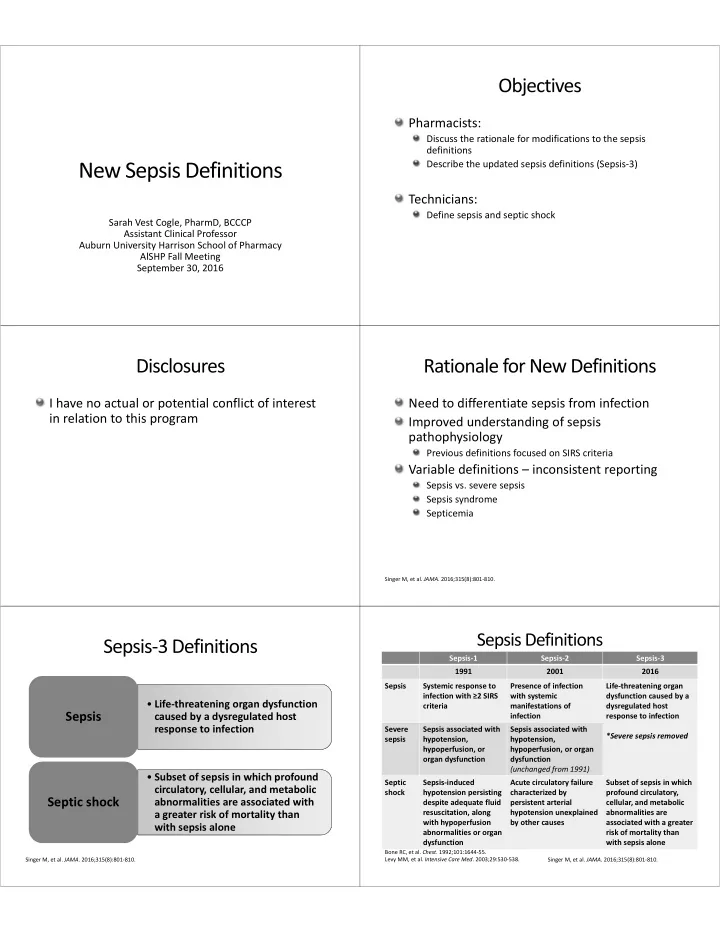
- Life‐threatening organ dysfunction
caused by a dysregulated host response to infection
Sepsis
- Subset of sepsis in which profound
circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone
Septic shock
Sepsis‐1 Sepsis‐2 Sepsis‐3 1991 2001 2016 Sepsis Systemic response to infection with ≥2 SIRS criteria Presence of infection with systemic manifestations of infection Life‐threatening organ dysfunction caused by a dysregulated host response to infection *Severe sepsis removed Severe sepsis Sepsis associated with hypotension, hypoperfusion, or
- rgan dysfunction
Sepsis associated with hypotension, hypoperfusion, or organ dysfunction (unchanged from 1991) Septic shock Sepsis‐induced hypotension persisting despite adequate fluid resuscitation, along with hypoperfusion abnormalities or organ dysfunction Acute circulatory failure characterized by persistent arterial hypotension unexplained by other causes Subset of sepsis in which profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone
Bone RC, et al. Chest. 1992;101:1644‐55. Levy MM, et al. Intensive Care Med. 2003;29:530‐538. Singer M, et al. JAMA. 2016;315(8):801‐810.