
SLIDE 1
1
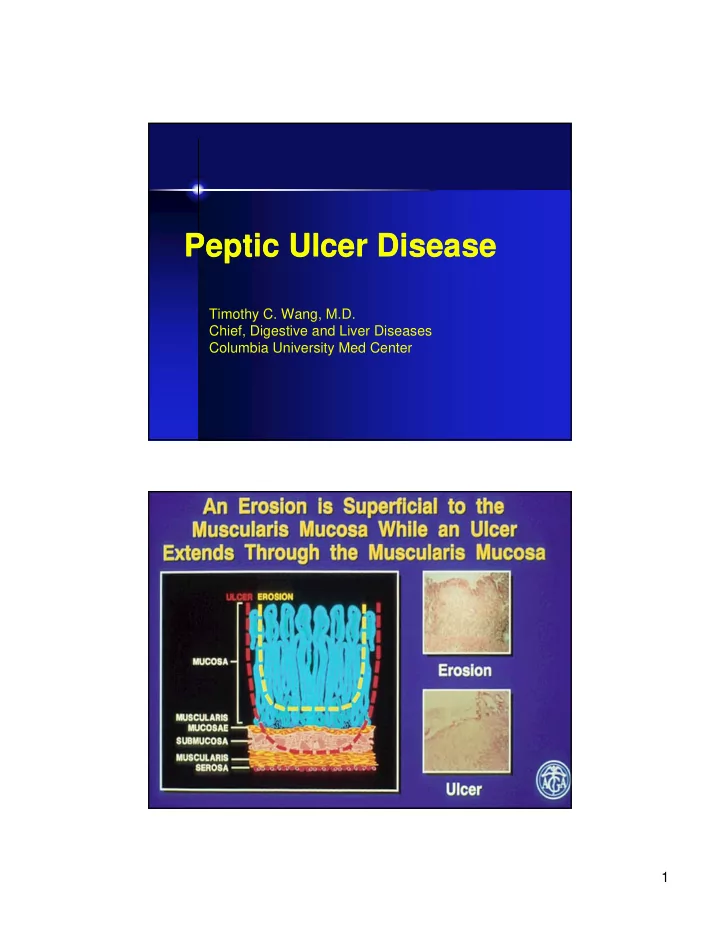
Peptic Ulcer Disease Peptic Ulcer Disease
Timothy C. Wang, M.D. Chief, Digestive and Liver Diseases Columbia University Med Center
Peptic Ulcer Disease Peptic Ulcer Disease Timothy C. Wang, M.D. - - PDF document
Peptic Ulcer Disease Peptic Ulcer Disease Timothy C. Wang, M.D. Chief, Digestive and Liver Diseases Columbia University Med Center 1 (body/corpus) (low acid) (antral) (high acid) 2 Simple versus Complicated Peptic Ulcer Disease
1
Timothy C. Wang, M.D. Chief, Digestive and Liver Diseases Columbia University Med Center
2 (low acid) (high acid) (antral)
(body/corpus)
3
– Symptomatic – Asymptomatic
– Bleeding – Perforation – Death
prevalence of 10%
common as GU
increases with age
declining Bleeding ulcer
4
5
6
7
8
pepticsches Geschwur”
acid is a factor in most patients with PUD
9
10
11
12
– cephalovagal and local intragastric reflex arcs
– endocrine (gastrin) or paracrine (somatostain, histamine)
– positive (+) factors - amines/amino acids, gastric distention – negative (-) factors - increased acid or low pH Histamine is the final common mediator of acid secretion
13
–basal acid secretion -vagal regulation
35-40%, vagal 50%, gastrin 5%, gastrin, a.a.
14
Bhaskar KR et al, Nature 1992;360:458
Protective Factors Mucous layer thickness pH gradient Cell membrane hydrophobicity Bicarbonate secretion Mucosal blood flow Cell renewal
Mucous layer
15
16
17
HCL HCL Acid and pepsin Acid and pepsin Stomach Stomach lumen lumen pH pH < < 2 2
Collins, 1990. Collins, 1990.
Protective factors: Protective factors: all are all are PG PG dependent dependent Mucous layer thicknes Mucous layer thicknes pH gradient pH gradient Cell membrane Cell membrane hydrophobicity hydrophobicity Bicarbonate secretion Bicarbonate secretion Mucosal Mucosal blood flow blood flow
Mucous layer Mucous layer Gastric Gastric epithelium epithelium Gastric pit Gastric pit HCL HCL
HCO HCO
3 3Š Š
HCO HCO
3 3Š Š HCO
HCO
3 3Š Š
HCO HCO
3 3Š Š
pH7 pH7
– Ion trapping: rapid, compound specific – Enterohepatic recirculation
– Systemic effect
– Increased neutrophil vascular adherence mediated by increased TNFα and ICAM
18
Schoen Schoen . . Am J Am J Med Med . 1989;86:449. . 1989;86:449.
pH = 2 pH = 2 Gastric Lumen Gastric Lumen pH = 1-2 pH = 1-2 AH AH A A–
– + H+
+ H+ AH AH A A–
– + H
+ H
+ +
A A–
– + H
+ H
+ +
AH AH AH AH A A–
– + H
+ H
+ +
Mucous Gel Layer Mucous Gel Layer pH = 7 pH = 7 pH = 7.4 pH = 7.4 Gastric Epithelium Gastric Epithelium Blood Blood pH = 7.4 pH = 7.4
NSAIDs NSAIDs Excreted Excreted in Bile in Bile Indomethacin Indomethacin Diclofenac Diclofenac Naproxen Naproxen Piroxicam Piroxicam Sulindac Sulindac Oxaprozin Oxaprozin Ketorolac Ketorolac
Liver Liver Gallbladder Gallbladder Reabsorption Reabsorption Absorption Absorption Stomach Stomach Reflux (with bile) Reflux (with bile) Intestinal Intestinal Damage Damage
19
Endothelial effects Endothelial effects
stasis ischemia ischemia
direct toxicity “ion trapping” “ion trapping” Epithelial effects (due to Epithelial effects (due to prostaglandin depletion) prostaglandin depletion)
_ HCl HCl secretion secretion
⎠ mucin mucin secretion secretion
⎠ HCO HCO
3 3 secretion
secretion
⎠ surface active surface active phospholipid phospholipid secretion secretion
⎠ epithelial cell proliferatio epithelial cell proliferation EROSIONS EROSIONS
ULCER ULCER
HEALING (spontaneous HEALING (spontaneous
Acid Acid
8 8Platelets Platelets 8 8Endothelium Endothelium 8 8Stomach Stomach 8 8Kidney Kidney 8 8Macrophages Macrophages 8 8Leukocytes Leukocytes 8 8Fibroblasts Fibroblasts 8 8Endothelial cell Endothelial cell
Physiologic Physiologic Stimulus Stimulus “Housekeeping” “Housekeeping” PGI PGI
2 2
TXA TXA
2 2
PGE PGE
2 2
COX-1 COX-1 Constitutive Constitutive Inflammatory Inflammatory Stimulus Stimulus PGI PGI
2 2
PGE PGE
2 2
COX-2 COX-2 Inducible Inducible Inflammation Inflammation
20
Discovery of human gastric bacteria
Rediscovery of gastric bacteria
Isolation and culture of C. pyloridis by Marshall and Warren
Eradication reduces DU recurrence
Bacteria are renamed H. pylori
Association of H. pylori with gastric cancer and MALT lymphoma
Complete genome sequence of H. pylori
Helicobacter pylori
21
industrialized nations
– Familial clustering (passed among siblings older-younger) – High rates in institutions with crowding & poor sanitation
Humans
Mouse
Ferret
Rat
Chicken
Hamster
Cat
Woodchuck
Gerbil
Dog
Other
22
Src
Shp-2
– Acid tolerant (urease, UreI) – Motile (multiple flagella)
– Attachment (32 Hop adhesins, including BabA) – Other virulence factors: VacA, picB/cagE – Genes regulated by slipped-strand mispairing – Uses molecular hydrogen for energy Type IV Secretion System
Early adulthood Childhood
Ingestion of H. pylori (gastroenteritis/diarrhea) Chronic, active gastritis
Late adulthood
Asymptomatic (90%)
MALT lymphoma (<1%)
Duodenal ulcer (5%)
Body gastritis
Gastric ulcer (3%)
Gastric cancer (0.5%)
Menetrier’s Hyperplastic polyps (<1%) Fe deficiency anemia
23
ALL HP INFECTIONS ARE NOT ALIKE: HISTOLOGY IS KEY
gastritis) without disease – Normal acid
– Increased acid (DU)
cancer)
metaplasia – Decreased acid (gastric cancer)
in hypochlorhydria
gastritis invariably present with H. pylori
established (Koch’s postulates):
– Eradication of H. pylori eliminates gastritis – Ingestion of H. pylori by 2 volunteers
usually asymptomatic
HP -infected patients.
(DU) & 80% (GU) patients.
prevalence of HP in PUD.
NSAID (-) ulcers.
markedly by HP eradication.
recur after HP eradication.
Duodenal Ulcer
Gastric Ulcer
24
– Role for incompletely processed gastrins
25
Increased gastrin-17
Low levels
(CagA, vacAs1, babA2)
26
Type I: Polypoid Gastric Cancer
Type II:Exophytic Gastric Cancer
Fox and Wang NEJM, 2001
27
tissue
rare tumor strongly associated with H. pylori infection
cell that eventually gives rise to MALT lymphoma (NEJM 1998)
regression of early MALT lymphomas in 60-92% of cases
are superficial (stage 1 T1) are most likely to respond to antibiotics
– Serology (ELISA, immunoblot) – UBT (C13 or C14)
– Rapid urease assay – Histology (Warthin-Starry, Giemsa, Immunohistochemistry – Culture, PCR analysis
– e.g. H. pylori stool antigen (HpSA)
28
89-95%
90-95%
87-91%
98% tetracyline)
90-95% clarithromycin)
(in >90%)
29
Ellison in 1955
“gastrinoma triangle”
– Duodenal wall - 40-50% – Pancreas - 20-25% – Stomach and jejunum - rare – Extrapancreatic, extraintestinal - 10-20%
(44%) to 20 cm
duodenal bulb
30