
SLIDE 1
5/28/2015 1
Pathophysiology of the digesti e s stem digestive system
Blagoi Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv
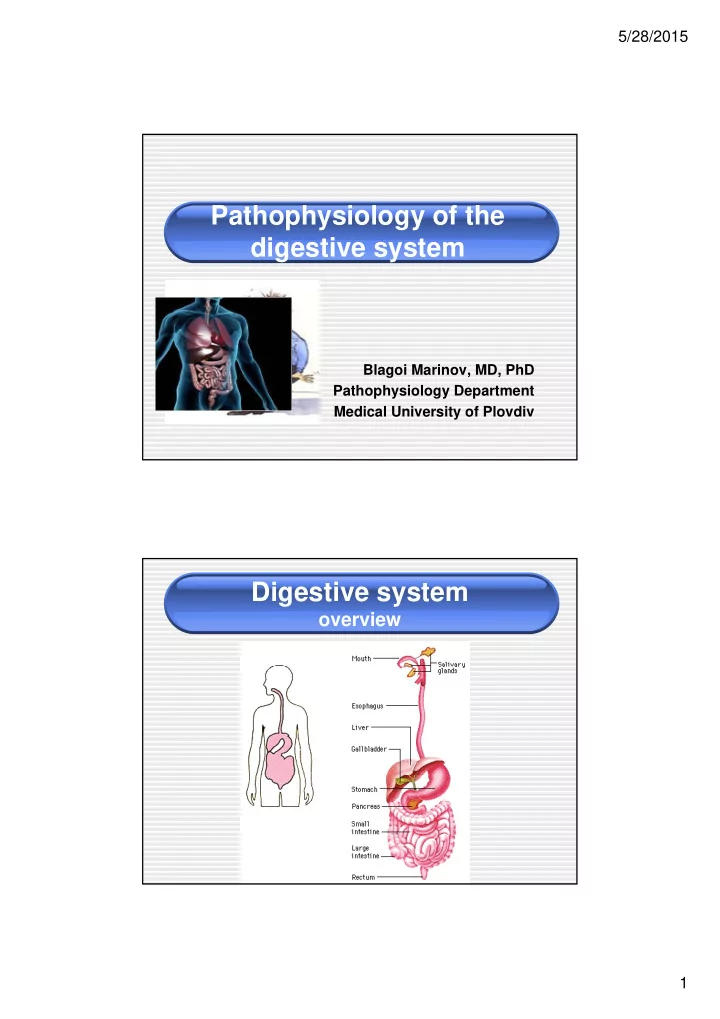
Digestive system
- verview
Pathophysiology of the digesti e s stem digestive system Blagoi - - PDF document
5/28/2015 Pathophysiology of the digesti e s stem digestive system Blagoi Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Digestive system overview 1 5/28/2015 Most frequent GI disorders Gastritis Peptic
Exogenous factors Endogenous factors Gastritis
substances
Bloodflow HCO3-
H.Pylori on the surface of gastric epithelial cells
Hypersecretion
ti NSAID
problems. Al h l i d ti
the brain to the stomach to reducing acid secretion.
produces a hormone that stimulates the stomach to secrete digestive produces a hormone that stimulates the stomach to secrete digestive
(pylorus) are enlarged, enabling contents to pass more freely from the
Pancreatitis is an inflammatory process in which pancreatic enzymes autodigest the gland. Acute pancreatitis occurs suddenly and lasts for a short period of time and usually resolves.
Severe Mild
80% of intussusception occur in children under 2 years
foramen of Winslow, and diaphragmatic hernias or postoperative secondary to mesenteric defects) N l ti
g
p
enteropathy/stricture