
SLIDE 1
4/13/2018 1
Drugs to Treat Obesity: Do They Work?
Sarah Kim, MD Associate Clinical Professor Division of Endocrinology UCSF Diabetes Updates 4/12/18
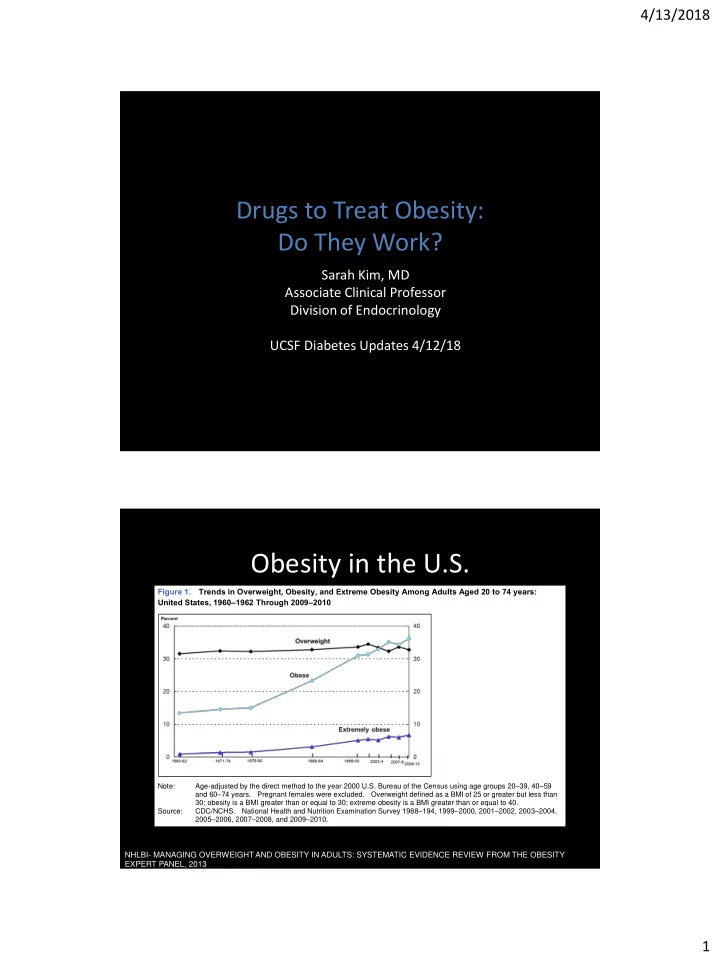
Obesity in the U.S.
” – – – – –
Figure 1. Trends in Overweight, Obesity, and Extreme Obesity Among Adults Aged 20 to 74 years: United States, 1960–1962 Through 2009–2010
Note: Age-adjusted by the direct method to the year 2000 U.S. Bureau of the Census using age groups 20–39, 40–59 and 60–74 years. Pregnant females were excluded. Overweight defined as a BMI of 25 or greater but less than 30; obesity is a BMI greater than or equal to 30; extreme obesity is a BMI greater than or equal to 40. Source: CDC/NCHS. National Health and Nutrition Examination Survey 1988–194, 1999–2000, 2001–2002, 2003–2004, 2005–2006, 2007–2008, and 2009–2010.
NHLBI- MANAGING OVERWEIGHT AND OBESITY IN ADULTS: SYSTEMATIC EVIDENCE REVIEW FROM THE OBESITY EXPERT PANEL, 2013