
MOL2NET, 2018, 4, http://sciforum.net/conference/mol2net-04 1
MDPI
MOL2NET, International Conference Series on Multidisciplinary Sciences
A Case Study of the Dietitian’s Role in Rehabilitation of Stroke Patients through Nutritional
Delia Alviarez a, Kathryn Ayres MA RD LDN b
a West Coast University b West Coast University
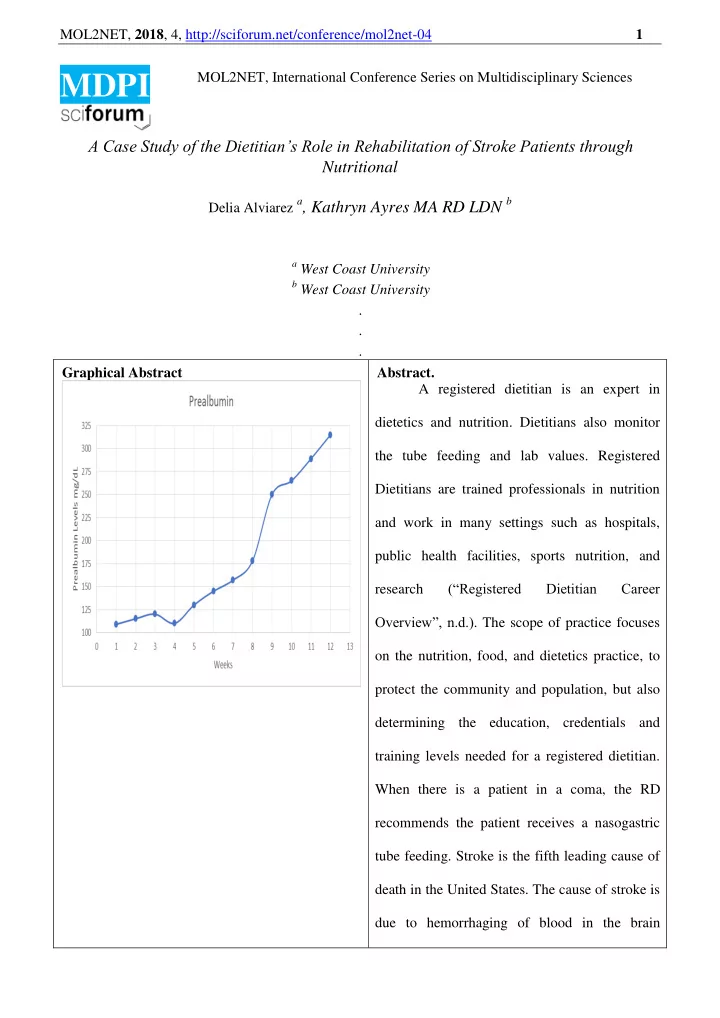
. . . Graphical Abstract Abstract. A registered dietitian is an expert in dietetics and nutrition. Dietitians also monitor the tube feeding and lab values. Registered Dietitians are trained professionals in nutrition and work in many settings such as hospitals, public health facilities, sports nutrition, and research (“Registered Dietitian Career Overview”, n.d.). The scope of practice focuses
- n the nutrition, food, and dietetics practice, to
protect the community and population, but also determining the education, credentials and training levels needed for a registered dietitian. When there is a patient in a coma, the RD recommends the patient receives a nasogastric tube feeding. Stroke is the fifth leading cause of death in the United States. The cause of stroke is due to hemorrhaging of blood in the brain