
SLIDE 1
Page 1
NEUROCRITICAL CARE PROGRAM
UC SF
Intracerebral Hemorrhage: Acute and Long-Term Blood Pressure Management
- J. Claude Hemphill III, MD, MAS
Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California, San Francisco Chief of Neurology, San Francisco General Hospital Past-President, Neurocritical Care Society
Disclosures Research Support: NIH/NINDS; Cerebrotech Medical Stock (options): Ornim
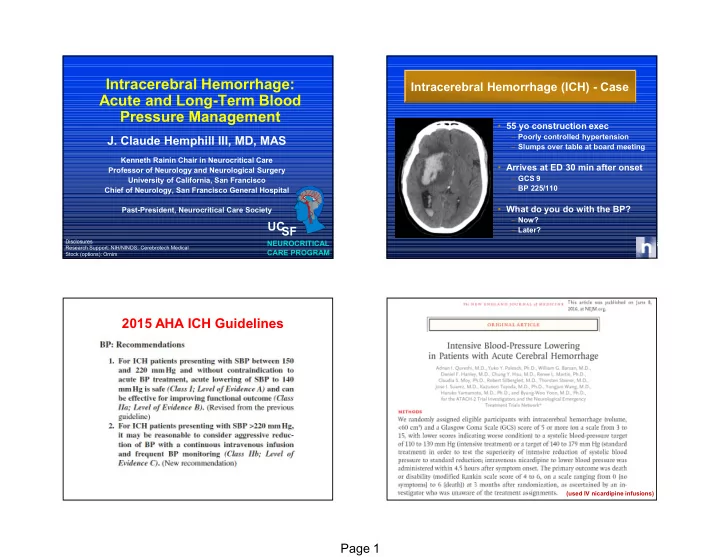
Intracerebral Hemorrhage (ICH) - Case
- 55 yo construction exec
– Poorly controlled hypertension – Slumps over table at board meeting
- Arrives at ED 30 min after onset
– GCS 9 – BP 225/110
- What do you do with the BP?
– Now? – Later?
2015 AHA ICH Guidelines
(used IV nicardipine infusions)