
7/28/2016
Integrated Behavioral Health Care via Telepsychiatry
Meera Narasimhan, MD Associate Provost University
- f South Carolina
& Professor and Chair Department of Neuropsychiatry and Behavioral Science USC-SOM
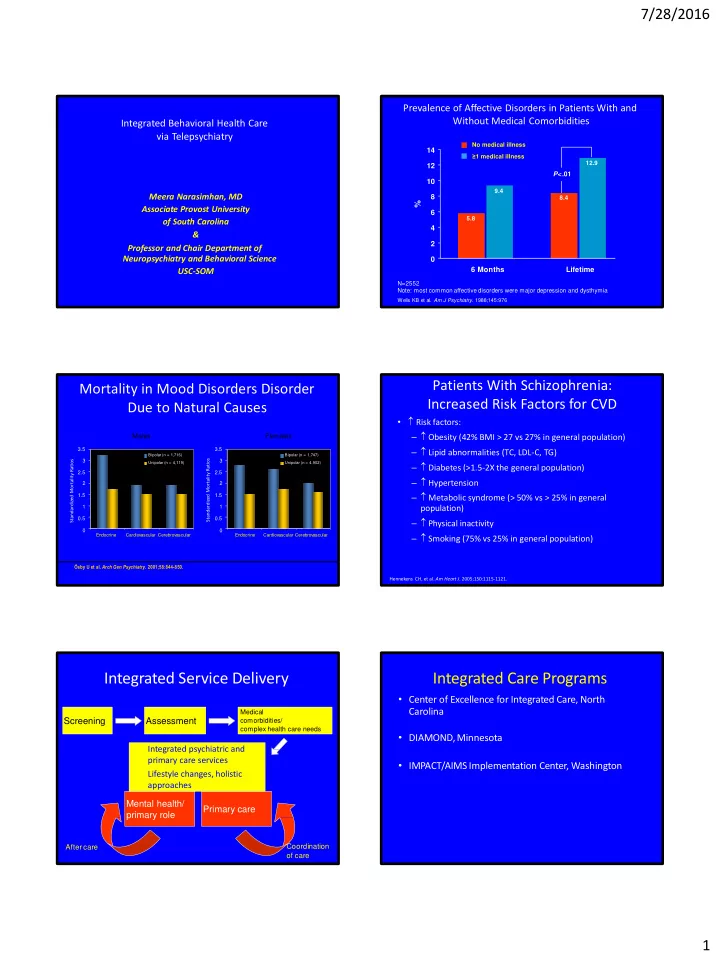
Prevalence of Affective Disorders in Patients With and Without Medical Comorbidities
N=2552 Note: most common affective disorders were major depression and dysthymia
Wells KB et al. Am J Psychiatry. 1988;145:976
2 6 4 10 8 12 14 6 Months Lifetime
No medical illness ≥1 medical illness P<.01
%
5.8 9.4 8.4 12.9
Mortality in Mood Disorders Disorder Due to Natural Causes
Males Females
2 1.5 1 0.5 3 2.5 3.5 3.5
Bipolar (n = 1,747) Unipolar (n = 4,902)
Ősby U et al. Arch Gen Psychiatry. 2001;58:844-850. Hennekens CH, et al. Am Heart J. 2005;150:1115-1121. Standardized Mortality Ratios Standardized Mortality Ratios 2 1.5 1 0.5 3 2.5
Bipolar (n = 1,716) Unipolar (n = 4,119) Endocrine Cardiovascular Cerebrovascular Endocrine Cardiovascular Cerebrovascular
Patients With Schizophrenia: Increased Risk Factors for CVD
- Risk factors:
– Obesity (42% BMI > 27 vs 27% in general population) – Lipid abnormalities (TC, LDL-C, TG) – Diabetes (>1.5-2X the general population) – Hypertension – Metabolic syndrome (> 50% vs > 25% in general population) – Physical inactivity – Smoking (75% vs 25% in general population) Assessment Primary care Mental health/ primary role
Medical comorbidities/ complex health care needs
Screening
Integrated Service Delivery
Integrated psychiatric and primary care services Lifestyle changes, holistic approaches
After care Coordination
- f care
Integrated Care Programs
- Center of Excellence for Integrated Care, North
Carolina
- DIAMOND, Minnesota
- IMPACT/AIMS Implementation Center, Washington