
SLIDE 1
2/16/2019 1
Pearls and Pitfalls in the treatment
- f Movement Disorders
A Case-based approach
Alberto J. Espay, MD, MSc Professor of Neurology Director and Endowed Chair James J. and Joan A. Gardner Family Center for Parkinson’s Disease and Movement Disorders University of Cincinnati Academic Health Center
52nd Annual Recent Advances in Neurology February 4-16, 2019 IUCSF, San Francisco
Initial and subsequent medication therapy of Parkinson’s disease
case 1
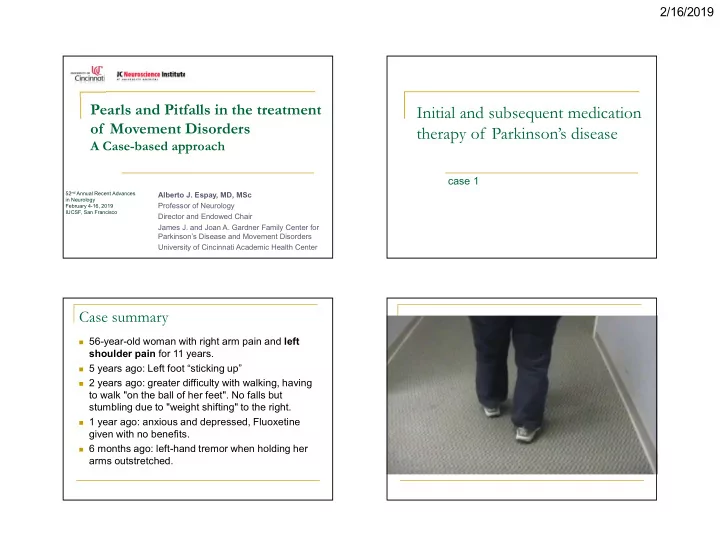
Case summary
56-year-old woman with right arm pain and left
shoulder pain for 11 years.
5 years ago: Left foot “sticking up” 2 years ago: greater difficulty with walking, having
to walk "on the ball of her feet". No falls but stumbling due to "weight shifting" to the right.
1 year ago: anxious and depressed, Fluoxetine
given with no benefits.
6 months ago: left-hand tremor when holding her