
SLIDE 1
3/26/2013 1
Infectious Diseases Review for the Family Medicine Boards 2013
Brian Schwartz, MD Assistant Professor UCSF, Division of Infectious Diseases
Overview
- Lecture Outline
– Cases with questions (90%) – High yield information (10%)
- Syllabus
– Answers to case questions with descriptions
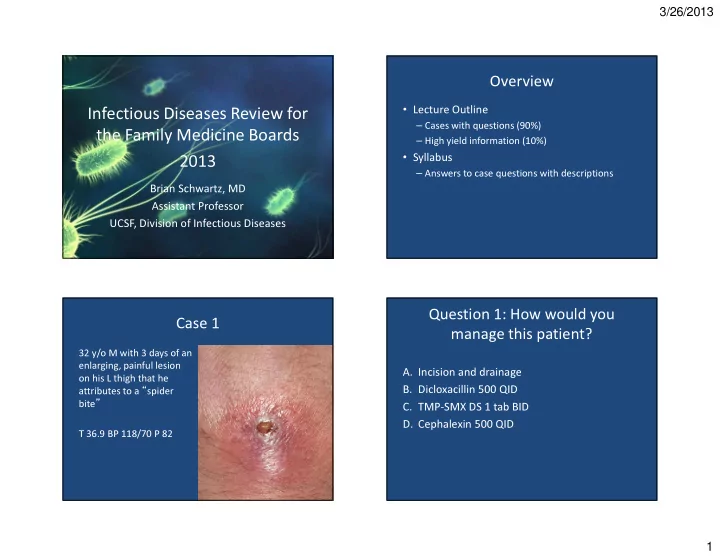
Case 1
32 y/o M with 3 days of an enlarging, painful lesion
- n his L thigh that he
attributes to a “spider bite” T 36.9 BP 118/70 P 82
Question 1: How would you manage this patient?
- A. Incision and drainage
- B. Dicloxacillin 500 QID
- C. TMP-SMX DS 1 tab BID
- D. Cephalexin 500 QID