
SLIDE 1
9/8/2012 1
Modeling of Inherited Arrhythmogenic Syndromes with Human Induced Pluripotent Stem Cells
Lior Gepstein. MD, PhD
Rambam Medical Center Technion - Israel Institute of Technology Disclosures: None
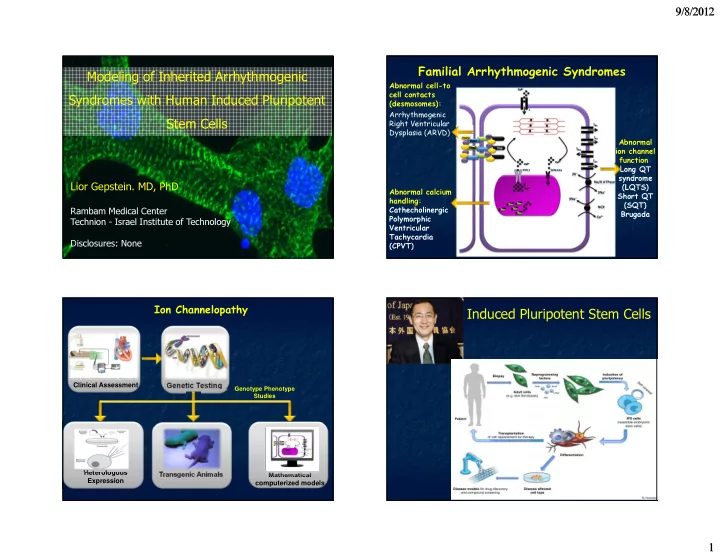
Abnormal cell-to cell contacts (desmosomes): Arrhythmogenic Right Ventricular Dysplasia (ARVD) Abnormal ion channel function: Long QT syndrome (LQTS) Short QT (SQT) Brugada Abnormal calcium handling: Cathecholinergic Polymorphic Ventricular Tachycardia (CPVT)
Familial Arrhythmogenic Syndromes
Ion Channelopathy
Clinical Assessment
Genetic Testing
Genotype Phenotype Studies
Mathematical computerized models Heterologous Expression Transgenic Animals