SLIDE 3 Nancy Moureau, BSN, RN, CRNI, CPUI, VA-BC 4/29/2012 3
Case Study
Situation – Friday 4pm PICC placement requiring confirmation prior to use
Background – 72 yo female requires PICC for fluids, K+ and medications. Radiologist leaves at 16:30, PICC nurse not authorized to read films. X-ray report dictated PICC in the IJ
Action choices
–
Remove (patient required access)
–
Wait for catheter to drop (no PICC nurse available S/S)
–
Pull back to alternative position (K+ is an irritant)
–
Replace with new insertion or exchange
Nurse pulled catheter back – no X-ray recheck
Response – LOC change within 24 hours, pt confused, died within 48 hours
Cause – Arterial placement
Potential for Malpractice – Radiologist misread film (too difficult to differentiate vein from artery up the neck – final report PICC in vertebral artery), Nurse did not correct
- r confirm the placement, cleared the line for use. Nurse suspended from work.
Patient’s family sued, hospital settled for undisclosed amount.
Solution – Better forms of confirmation that allow location pinpoint during insertion, and vein and artery differentiation.
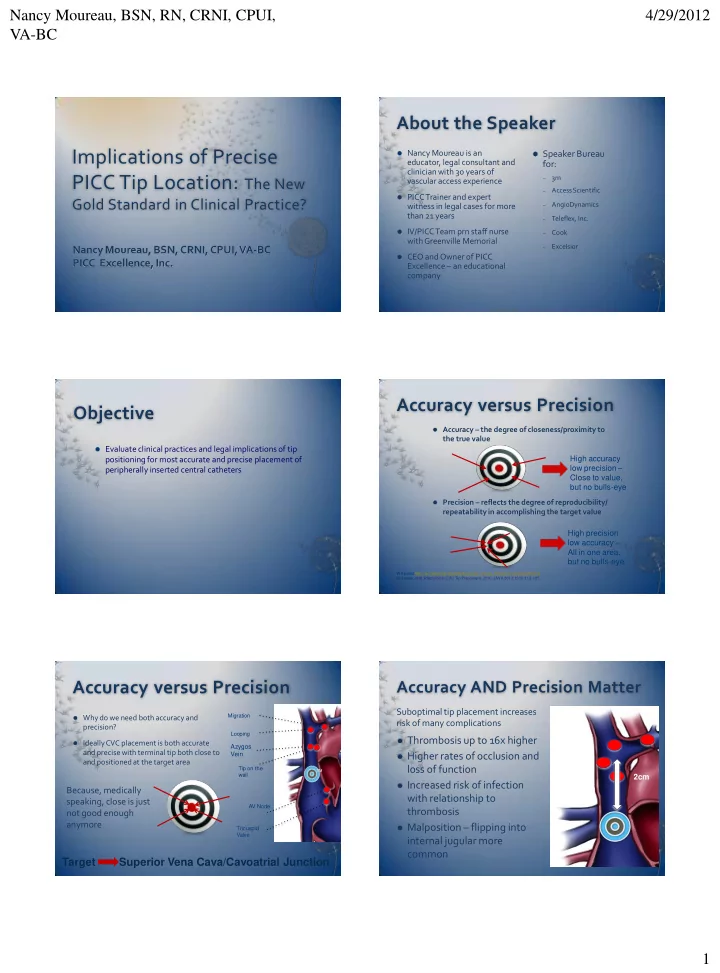
Target Area Superior Vena Cava/CAJ
- Cardiac Arrythmias
- Arterial Access
- Erosion through vein wall
- Thrombosis
- Erosion through heart wall
- Pulmonary Emboli
- Cardiac Tamponade
Complications
- Positioning too deep, malposition or in artery
- High position of terminal tip
Left sided position without making downward turn into SVC
- Irritation to vein wall. Suboptimal position high in SVC,
subclavian or collateral veins
- Positioning in the right atrium or ventricle
- Coagulation and thrombotic development resulting in emboli
blocking pulmonary artery into lungs
- Erosion of catheter through heart wall allowing infusion of
solutions into the pericardium
Cause
- Atrial fibrillation, flutter, premature ventricular contractions , emboli, stroke
- Infusion into pleural space.
- Failure to achieve blood return
- Pneumonia, infiltrates, abscess
- Poor function, lack of blood return, pulmonary emboli, post thrombotic
sequellae
- Compromise of heart function, cardiac tamponade with 70% mortality
- Difficulty breathing, chest pain, palpitations and sudden death
- Pericardial effusion results in pressure on the heart resulting in decreased
cardiac function and death
Result
Measuring Liability
15
Levels of success with Landmark: 46-75%2,3,4,5 Success with Magnetic navigation: 80%3 Success with ECG: 55-88%6,7 Since SA node is located near the CAJ in the
posterior wall of the right atrium, the P-wave acts like a beacon used to guide a catheter tip, towards the CAJ
ECG and Doppler potential success 95% or
greater8
References:
- 2. Trerotola et al. J Vasc Interv Radiol 2007; 18:513-518
- 3. Naylor JAVA 2007; 12:1:29-31
- 4. VSN Market Research
- 5. Hostetter, R. et al JAVA 15:3, 114-123
- 6. Starr et al, Ann Surg, 1986; 673-676
- 7. Salmela et al. Acta Anaesthesiol Scand 1993; 37:26-28
- 8. Clinical data on file at VasoNova, Inc.
Liability Issues
Performing tip confirmation: Where is the risk? Where is the safety?
X-ray – The Current Standard
- Simple chest X-ray confirmation
- Frequently difficult to read
- General area validation. Placement
frequently too deep or too shallow (10-15%)
- Malpositions: 5-8% in IJ, 3-5%
contra-lateral or “looped back”
- 1D flat film reading missing Azygos
and other malpositions
- More than 50% need some kind of
adjustment after first placement
- Failure to differentiate arterial
placement
ECG Confirmation
- Greater accuracy and precision
- Requires discernible P-wave and
interpretation
- Measures changes in P-wave once
reaching superior vena cava
- Requires understanding of
P-wave polarization and depolarization
- Unable to detect arterial placement
- Improved accuracy and precision
ECG with Doppler Confirmation
- Same advantages as with ECG
- Indicates position or malposition
with flow indicator
- Detects arterial flow
- Combined use designed to measure
target location and provide all clear Blue Bullseye indication
- Broad application for accuracy and
precision with cardiac patients
- No interpretation required
Reducing Potential for Malpractice
How can you effectively reduce the potential for malpractice?
By developing processes that promote consistent outcomes
greater than 95% of the time
Provide confirmation in timely manner with insertion while ruling
Put the tools in the hands of the inserter
X-Ray – General location for terminal tip – Accurate most of the time – Is that good enough? ECG/EKG – Greater accuracy and precision, applicable to most patients with P-wave ECG/EKG + Doppler – Achieves maximum accuracy, precision and safety, greatest application
Doppler Principles for Tip Position
Flow in veins is pulsatile driven by heart cycle hemodynamics
Systolic inflow Diastolic inflow Atrial Contraction
S D A
SVC Pulse Doppler