
SLIDE 1
5/26/2017 1
Gastric Polyps:
Diagnosis and Management
Gregory Y. Lauwers, MD Senior Member
- H. Lee Moffitt Cancer Center & Research Institute
Tampa, FL Gregory.Lauwers@Moffitt.org
- “I have no relevant relationships
requiring disclosure”
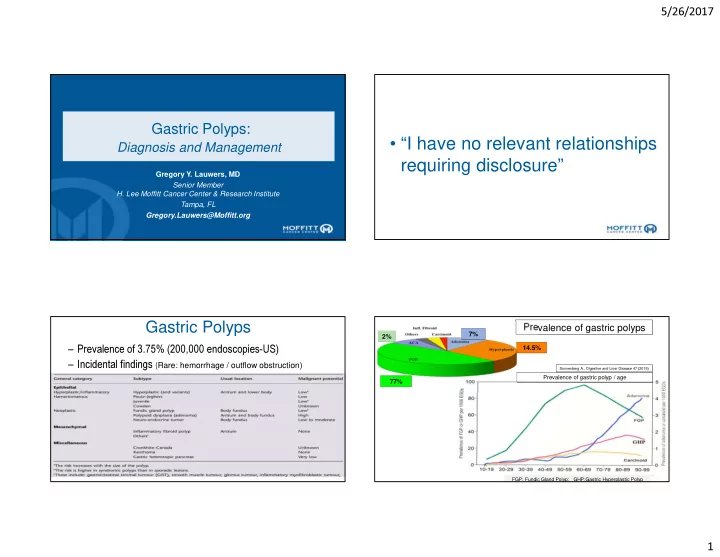
– Prevalence of 3.75% (200,000 endoscopies-US) – Incidental findings (Rare: hemorrhage / outflow obstruction)
Gastric Polyps
Prevalence of gastric polyps
FGP: Fundic Gland Polyp; GHP:Gastric Hyperplastic Polyp
77% 14.5% 7% 2%
Prevalence of gastric polyp / age
Sonnenberg A., Digestive and Liver Disease 47 (2015)