SLIDE 6 9/30/2016 6
So why does your patient have a BP of a 60 yr old?
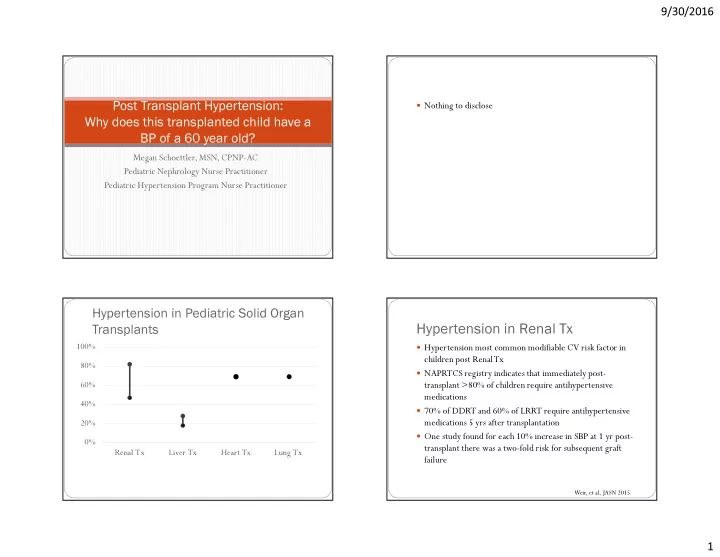
Look at the prevelance of the specific solid organ transplant Multifactorial but could be due to medication, decreased
renal function, fluid overload or obesity
You diagnosed with a 24 hrABPM You can treat based on the underlying pathology Monitor with yearly with ABPM and ECHO
Resources
- Basiratnia, M., Esteghamati, M., Ajami, G.H., Amoozgar, H., Cheriki, C., Soltani, M., Derakhshan, A.,
Fallahzadeh, M.H. (2011). Blood pressure profile in renal transplant recipients and it relation to diastolic function:tissue Doppler echocardiographic study. Pediatric Nephrology, 26, 449-457.
- Bjerre A, TangeraasT, Heidecke H, Dragun D, Dechend R, Staff AC.(2016) Angiotensin II type 1 receptor
antibodies in childhood kidney transplantation. Pediatric Transplant , 20, 627– 632.
- Cochrane Review: Pharmacological interventions for hypertension in children Chaturvedi S, Lipszyc DH,Licht C,
Craig JC, Parekh RS. Pharmacological interventions for hypertension in children. Cochrane Database of Systematic Reviews 2014, Issue 2. Evid.-Based Child Health 9: 581–583 (2014)
.L., Carpenter, A., Rankin, S., De Angelis, M., Avitzur, Y., Mouzaki, M. (2015). Overweight, central obesity, and cardiometabolic risk factors in pediatric liver transplantation. Pediatric Transplantion, 19 175- 181.
- Dipchand, A.I., Kirk, R., Mahle, W
.T., Tresler, M.A., Naftel, D.C., Pahl, E., Miyamoto, S.D., Blume, E., Guleserian, K.J., White-Williams, C., Kirklin, J.K. (2013). Ten yr of pediatric heart transplantation: A report from the Pediatric Heart Transplant Study. Pediatric Transplantation, 17, 99-111.
- Filler G, Melk A, Marks SD. (2016) Practice recommendations for the monitoring of renal function in pediatric
non-renal organ transplant recipients. Pediatric Transplant, 20,352– 363.
- FLYNN JT, DANIELS SR, HAYMAN LL, et al. Update: Ambulatory blood pressure monitoring in children and
adolescents: A scientific statement from the American Heart Association.Hypertension, 63: 1116–1135.
Resources Continued
- Garcia-Bello, J.A., Romo-Del Rio, E.G., Mendoza-Gomez, E., Camarena-Arias,P
.A. (2016). Effect of Immunosuppressive Therapy on Cardiovascular Risk Factor Prevalence in Kidney-transplanted Children: Comparative Study. Journal of Transplantation proceedings, 48, 639-642.
- Hamdani G, Nehus EJ, Hooper DK, Mitsnefes MM. (2016)Masked hypertension and allograft function in
pediatric and young adults kidney transplant recipients. Pediatric Transplant , 00: 1– 6.
- HAMDANI G, NEHUS EJ, HANEVOLD CD, et al. Ambulatory blood pressure, left ventricular
hypertrophy, and allograft function in children and young adults after kidney transplantation.Transplantation
- KDIGO (2012) Clinical practice guideline for the management of blood pressure in chronic kidney
- disease. www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO_BP
- Kirkby, S., Hayes, D. (2014). Pediatric lung transplantation: indications and outcomes. Journal of Thoracic
Disease, 6(8), 1024-1031.
- Koomans, H.A., Ligtenberg, G. (2001). Mechanisms and Consequences of Arterial Hypertension After
renal transplantation. Transplantation, 6(72), S9-S12.
- Matloff, R.G., Arnon, R. (2015).
The Kidney in Pediatric Liver Disease. Current Gastroenterology Reports, 17(36), 1-9.
V .A., Anand, R., Daniels, S.R., Yin, W ., Alonso, E.M., SPLIT Research Group. (2012) American Journal of Transplantation, 12, 183-190.
- Mitsnefes, M.M., Portman, R.J. (2003). Ambulatory blood pressure monitoring in pediatric renal
- transplantation. Pediatric transplantation, 7, 86-92.
Resources Continued
- Naesens, M., Kuypers, D.R.J., Sarwal, M. (2009). Calcineurin Inhibitor Nephrotoxicity. American Society of
Nephrology, 4, 481-508.
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Chidren,
- Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and
- adolescents. Pediatrics,114, 555–576.
- Paripovic, D., Kostic, M., Spasojevic, B., Kruscic, D., Peco-Antic, A. (2010). Masked Hypertension and hidden
uncontrolled hypertension after renal transplantation. Pediatric Nephrology, 25, 1719-1724.
- Perito ER, Glidden D, Roberts JP
, Rosenthal P . Overweight and obesity in pediatric liver transplant recipients: Prevalence and predictors before and after transplant, United Network for Organ Sharing Data,1987– 2010.Pediatric Transplantation, 16, 41–49.
- Perito, E.R., Rhee, S., Glidden, D., Roberts, J.P
., Rosenthal, P . (2012). Impact of the Donor Body Mass Index on the Survival of Pediatric LiverTransplant Recipients and Post-transplant Obesity. LiverTransplatation, 18, 930- 939.
- Roche, S. L., Kaufman, J., Dipchand, A.I., Kantor, P
.F., (2008). Hypertension After Pediatric Heart Transplantation is Primarily Associated with Immunosuppressive Regimen. Journal of Heart and Lung Transplantation, 27, 501-507.
- Sinha, M. D., Kerecuk, L., Gilg, J., Reid, C.J.D. (2012). Systemic arterial hypertension in children following renal
transplantation: prevalence and risk factors. Nephrology Dialysis Transplantation, 27, 3359-3368.
- Sinha, M. D., Kerecuk, L., Gilg, J., Reid, C.J.D. (2012). Progression to hypertension in non-hypertensive children
following renal transplantation. Nephrology Dialysis Transplantation 27, 2990-2996.