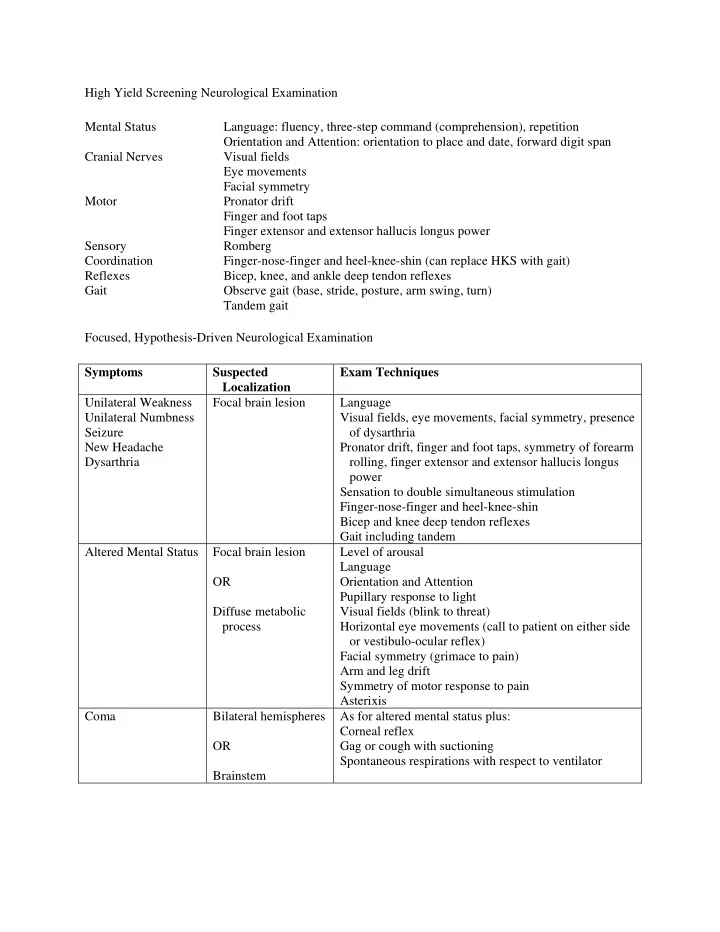
SLIDE 1 High Yield Screening Neurological Examination Mental Status Language: fluency, three-step command (comprehension), repetition Orientation and Attention: orientation to place and date, forward digit span Cranial Nerves Visual fields Eye movements Facial symmetry Motor Pronator drift Finger and foot taps Finger extensor and extensor hallucis longus power Sensory Romberg Coordination Finger-nose-finger and heel-knee-shin (can replace HKS with gait) Reflexes Bicep, knee, and ankle deep tendon reflexes Gait Observe gait (base, stride, posture, arm swing, turn) Tandem gait Focused, Hypothesis-Driven Neurological Examination Symptoms Suspected Localization Exam Techniques Unilateral Weakness Unilateral Numbness Seizure New Headache Dysarthria Focal brain lesion Language Visual fields, eye movements, facial symmetry, presence
Pronator drift, finger and foot taps, symmetry of forearm rolling, finger extensor and extensor hallucis longus power Sensation to double simultaneous stimulation Finger-nose-finger and heel-knee-shin Bicep and knee deep tendon reflexes Gait including tandem Altered Mental Status Focal brain lesion OR Diffuse metabolic process Level of arousal Language Orientation and Attention Pupillary response to light Visual fields (blink to threat) Horizontal eye movements (call to patient on either side
- r vestibulo-ocular reflex)
Facial symmetry (grimace to pain) Arm and leg drift Symmetry of motor response to pain Asterixis Coma Bilateral hemispheres OR Brainstem As for altered mental status plus: Corneal reflex Gag or cough with suctioning Spontaneous respirations with respect to ventilator
SLIDE 2
Vertigo Imbalance Brainstem or cerebellum OR Inner ear Detailed cranial nerve exam with special attention to the following: Horner’s syndrome Unidirectional vs. gaze-evoked nystagmus Vertical nystagmus Head thrust maneuver Pronator drift, finger and foot taps, symmetry of forearm rolling, finger extensor and extensor hallucis longus power Sensation intact to light touch in all four limbs Finger-nose-finger and heel-knee-shin Gait including tandem Dix-Hallpike maneuver Back Pain Bowel or Bladder Incontinence Bilateral Leg Weakness or Numbness Spinal cord Pronator drift, finger and foot taps, symmetry of forearm rolling Muscle tone in the legs Strength of deltoids, biceps, triceps, finger extensors, iliopsoas, quadriceps, hamstrings, foot and toe dorsiflexion Sensory level on trunk Rectal tone Diffuse Weakness High spinal cord, neuropathy, neuromuscular junction, or myopathy Pupillary response to light Eye movements, presence of ptosis Facial strength (check for bifacial weakness) Count to 30 in one breath, check NIF and FVC Strength of neck flexion, neck extension, deltoids, biceps, triceps, finger extensors, iliopsoas, quadriceps, hamstrings, foot and toe dorsiflexion Sensory gradient to pain from feet to thighs Sensory level on trunk Romberg Bicep, knee, and ankle deep tendon reflexes Ability to stand without using arms, walk on heels and toes *NIF = negative inspiratory force (normal < -60 cm H2O); FVC = forced vital capacity (normal > 2.0 L)
SLIDE 3 Key Teaching Points in Localization Weakness Pattern of weakness Tone Bulk Reflexes Sensory Loss Other Upper Motor Neuron Pyramidal Spastic Normal Increased Varies Anterior Horn Cell Pyramidal or myotomal Spastic or normal Atrophy Increased or decreased None Fasciculations Peripheral Nerve In distribution
nerve Normal or reduced Atrophy Decreased Prominent Neuromuscular Junction Diffuse Normal Normal Normal (myasthenia)
(botulism) None Ptosis and
paresis Muscle Proximal > Distal Normal Normal or patterned atrophy Normal None Aphasia Fluency Repetition Comprehension Expressive (Broca’s) Impaired Impaired Intact Receptive (Wernicke’s) Intact Impaired Impaired Global Impaired Impaired Impaired Conductive Intact Impaired Intact References: Kamel et al, A randomized trial of hypothesis-driven vs screening neurologic examination. Neurology Oct 2011, 77(14) 1395-1401.