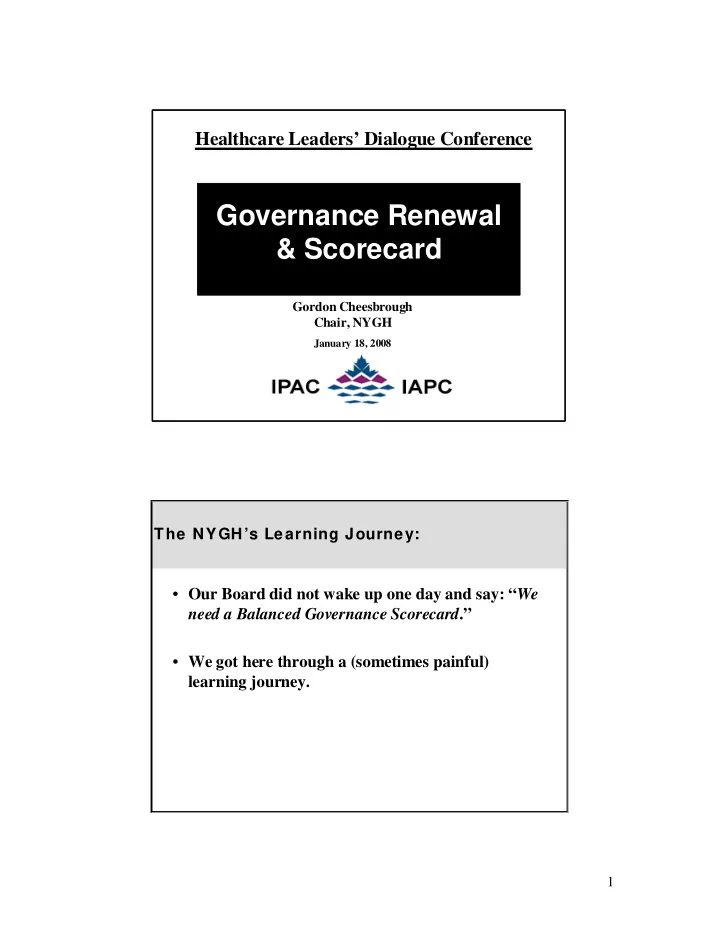
SLIDE 10 Gov erna nc e f or a communit y te ac hing hospita l in a c ontinuum of healt h care, prov iding compa ssionate and qualit y c are t o dive rse communitie s in Nort h Toront o and beyond – crea ting a de st ina tion of choic e f or patie nts, employe es, phys icia ns and v oluntee rs Pati ent/ Fam ily:
i le Quality Care & Patient S a f ety
as the A irline I ndustr y
ar e
- - Hi ghest S tandar d of Pat ie
n t Safety
i le Patient Exper ie n c e
- - Best Exp erience in Peer Group / Indu str y
( or Best “Possible”?)
- Pr ovider Destinati on of Ch oice
- Tim ely Access to Care
- Inf orm ation Exchange & Invo lvement in
Decision Making
- Patient /Family Driven: Responsive to
Needs, Values, Pr iorit ie s, Wishes
achin g Hospital Citizenry/ Comm un ity:
- Con fidence in Health Care P rovided
- Health Car e
S ervices Perceived as Ef fective & Eff icient to Meet Needs
am less Customer Exper ie n ce Acr oss th e HC System/ Cont inuum – Na vi gation & Coord ina t ion – Easier Mo ve m ent
- Linkages with the Com munity to Focu s on
Illness Prevent ion
n the Continuu m
- P rovide P atients/Famil ies wit h Right
Serv ic e, at Righ t Tim e, with Right Pro vider, I n Right P lac e, at t he Right Cost
- Ensure Collabor ation wit h Other P rovid e
r s & In tegration o f Ser vice s to C u st omers Overall H ospit al Cult ure:
- Ensure a Cultu re of H igh Perf orm ance
:
- - High Emplo yee Satisfaction
- - High Collabo rative
- - Continu ous I mpr ovement
- - Re
spect
Pub lic Awareness & Recogni tion: (includ es LHIN , Gov. , Co mmunity, Physici ans, Empl
s, B anker s, Donor s, Peer s/ Other Hospitals & B
ds)
- Known by All Key Stakeho lders for High Qualit y of
Care
ally Re spo nsib le W a y
- A Leading I nstitutio n/Le
ader & Role Model
- Awareness/Recognit ion of Our Brand
- An Inn ovator/ C
- ntribu tor:
- - Continu al Learnin g & Le
ad e r sh ip
- - Pr oactively Engaged with t he HC System
- - A Collabor ative Part ner wit hin & across LH IN
Boun daries
- - A Sy stem Integr ator
- - Net In tellec
t ual Contr ibutor to A S ust a in able & Viable H C S ystem
- - Contr ibute to Br oader Comm unity – Glo bal Re
ach (e .g.., Inf ec t ions, Pr oducts/ Ser vic es)
- - Great A lliance Partner
- - Health Care Deliver y (e.g.., Lean/ S ix Sigm a)
- - Balanced Governance S c
- recard
- Great Place to Wo rk – A Destinatio n of Ch oice
f or Employ e es & Ph ysic ian s Fin ancial:
- St rong F inancial Per for mance & Positio n –
Fisca l He a lth – Balance d B u dget
esour c es Directed t o Ne ed s/P rior ities (Equipm e n t, People, Services)
- Effective, Eff icient & Judicio us Allocation
- f F inancial Re
sou rces
ver aged Resou rces
- In ternal S taff S atisfied with Re
sour ces
- In crease F unding Avail a
b ility
LHIN/ Gov e rn ment :
- Establish Clear Accoun ta
b ility Agr ee m ents with the LHIN
u ild St rong Relation ship s wit h the LHIN & MOHLTC
Ends to Be Achieved Process Capabilities Required
S trateg y & Vi si on:
t ive l y Parti cipate in the D e velop ment o f, then App rove, Vision, S trategy , Targets & K e y Init ia t ives
- Oversee Execut ion of Strat e
gy
j or F inancial Decisio ns Fou ndat ion:
Ho sp ital Fou ndation Eff orts in S uppo rt of Hospital S trategic Ob jectives L H IN:
- Su pport the Development
- f
Partn e r sh ips & Int e gr ation I nitiatives
solut ion of C r oss LHIN Issu e s
- Su pport Other LHIN Key I nitiati ve
s Com m unicat ion/ Comm un ity:
- Pub licly Sup port the Hospital & Management
Tea m
- Commu nicate/Mar ket/Su pport the B
r and
an Advocate for the Hospital
- En su re Pro ductive, Ef fective Two-W a
y S takeholder C
C
P atients/ Fam ilie s
- Wor k to St rengthen Comm unity & Other Key
S takeholder R elatio nsh ips
Co mmunit y in Understand ing Health Care Needs & Healthcar e S ystem Plan ning & P rior ity S etting Qu ality:
- Assure/ Over see Qualit y:
- - Physicians
- - Practices/ Pr ocesses
- - R
esults
y Init iatives
- - Mo nitor & Evalu ate Patient
Safet y Im provem e n ts Fi nancial :
- Responsible & Thought ful Oversigh t of
Financial Reso urces
- App ropr iate Policies, Contr ols &
Practices for Financial P lanning & Managem e n t – Fiscal Polic ie s
t ing & Capital Budgets
- Assure Accuracy of Finan c
ial Inf ormat ion
n age m ent Pr actice s & Appro ve Audited F inancial Statem e n ts
l Perf orm a n c e
E nablers
Board Inf ormat ion R e q uirem e n ts:
cess to Str ategic Inf orm a t ion
essible, Use ab le , R elevant Info rmatio n Tools & Sy stem s to Suppo rt Gover nance Obj e ctiv e s Board Mem bers/ Le ad er s:
t ion, Mix, Evaluation o f Board Memb e r s
- I nvest in the Gr owth of the Board: O ngoing
Board Trainin g & Developm e n t
ct ion of B ehavior al Str engths, Skil ls, Knowledg e & Exp e r ience Ne ed e d to Sup port t he Hospital Vision & Str a t egy
- - Variety o f Perspectiv e
s
h ange
atio n
- - Evaluatio n
- - S uccession P lanning & Re
cr uitmen t
ct ive s & P rovid e for Eng a gem ent/ Par ticipation, Ro bust Discussions, Re spon sib le Decision Making , a s well as Ef ficiency
- Al ign Comm ittee Str ucture to Strategic
Them e s/ Ob jec t ives
r nance Focused vs. Operation Governa nce Stru cture & Processes:
- A ssess Board P erfo rmance: I ndividu a
l Members, Comm ittees, F ull Board
alan c ed G overnance Scor ec ar d Aligned w ith Hospital Balanced Sco reca r d
- I ntegrate Go vernance Pr ocesses wi th Hospital
St rategy Management S ystem
t e Boar d Str uctur e s & P rocesses Consist e n t with Best Pr a ct ice s:
e
- - Compo sitio n (inclu de Ex- Officio ,
Commu nity Reps)
- - Comm ittee: #, Desi gn, Fun c
t ions, Mem bers
etin g Durat ion & F requency
Governan c e Cu ltu r e:
- Wor k in Par tnership wit h Man a
gem ent to Nurtu re an En vironm e n t of:
- - Learnin g & Developm ent
- - H igh Per form ance
- - Col la
b oration
- - Risk Management
- - Mut ual Acc
- untability
- - Mut ual Re
spect and Trust
- - Recognit ion/ Ackno wledgement
- - P rod uctive Use o f Time
- - S afety & Security
Hospit al St aff :
- Ensure an Enviro nment of Safety ,
Securit y, Rec
Development
- S tron g, Positive Relationship s wit h All HC
Pr ofessio nals
- Well Designed Safe Wor kplace
Physicians:
n ce Deep I nvolvemen t in Hospital S trategy F orm ulation & Ex ec u tion
- A Pipeline of highly c
- mpetent
Phy sician Leaders
- S tro ng, Positive Relation ship s wit h
Phy sicians
- NY GH Perceived t o be Phy sician
Fr iendly Hosp ital Leadershi p/Manag ement :
- A Pipelin e
- f High ly Competent &
Comm itted Le ad e r s at Every Level
S tro ng Hospital Le ad e r sh ip & Management Risk Managem ent & Comp liance:
r prise Risk Manage m ent & Comp liance ( En sur e Compliance & P revention & Managem e n t of Risks)
pu tation
- Compliance with Bank Ag reements &
Covenants
b ility & Transparency
ar & Reliable Disclosures
r e
- Ensur e Approp riate Commu nica
t ion with Key S takeholders & F under s In format ion Managem ent:
Deve lo pment o f In form ation System Po licies & Practices Physicians:
r with P hysicia n s in Plannin g & Decision Making to Tap Collective Wisdom
r se e/Ap prove P hysician Staf fing/ Credent ia lin g
r se e P hysicia n Talent Managemen t & Leadership Developm ent
- Suppo rt Ph ysician F riend ly Practices
- Ove
r se e P rocess f or S elec t ion of Medical Leadership Hosp ital Hum an Resources (Ov e rall ):
Emp loyee Hea lt h & Saf ety
esource St rategy & Oversee Ex e cu tion
O verall HR P la n ning, Talent Management, P erfor mance Ma n a g e m e n t, Developm ent & S ucce ssion Risk Manag ement & Com plian ce:
Enter prise Risk Management Ef fort (Risk Analysis, e t c . )
- Actively Manage Risk & Regulator y Complian c
e
- Comm unication wit h Stakehold ers C
- n sistent with
the Accountabilities to Them
- Ensu re Appr opriate P rocesses in Place to Ensure
C
- m pliance with Legal Requirem e
n ts
- Oversee Em ployee Health & S afety
Hosp ital M anagem e n t/ Leadershi p:
Talent Management/ S ucce ssion P la n ning/ Leadership Developm ent fo r Key Lea d e r sh ip P ositions (CEO, COS/CMAC, Other S r. & P hysician Leader s)
w, Re cogn ize / Acknowledge & Reward Executive P e r for mance
r uit, S e lect, Coach, S uppor t, Evaluate, Compensate CEO & COS/ CMAC
- Hold Management Accoun ta
b le for Out comes
w/ Appro ve C EO & COS /CMA C P e r for mance Plans (Accou ntability Agr ee m ents)
- Live the Values of Listening, Learning ,
Leading, S erving
u lture: Ethics, P rinciples, Values, Coll a b oration , Stewardship , Open
f e Place for Due Diligen c e: P rob ing, Quest ions
b ility & Tru st
GOVERNANCE DESTINATION IN TWO TO FIVE YEARS