
SLIDE 1
4/18/2015 1
EXERCISE INDUCED LEFT ARM SWELLING
Bala Ramanan, MBBS 1st year vascular surgery fellow
INTRODUCTION
- The incidence of thoracic outlet syndrome (TOS) is approximately 0.3-
2% in the general population.
- The most common age range is 25 to 40 years.
- Venous TOS accounts for 2-3% of cases.
- Controversies in the management involve what treatment should be
done immediately and which type of treatment should be implemented.
Case Presentation
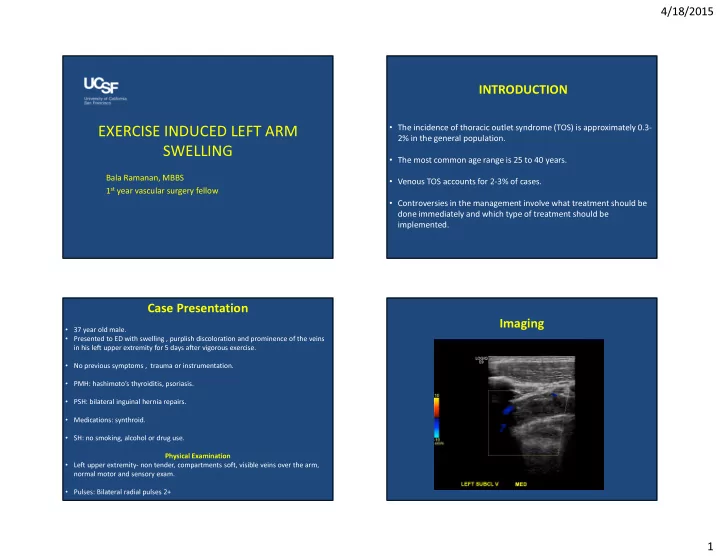
- 37 year old male.
- Presented to ED with swelling , purplish discoloration and prominence of the veins
in his left upper extremity for 5 days after vigorous exercise.
- No previous symptoms , trauma or instrumentation.
- PMH: hashimoto’s thyroiditis, psoriasis.
- PSH: bilateral inguinal hernia repairs.
- Medications: synthroid.
- SH: no smoking, alcohol or drug use.
Physical Examination
- Left upper extremity- non tender, compartments soft, visible veins over the arm,
normal motor and sensory exam.
- Pulses: Bilateral radial pulses 2+