
SLIDE 1
Examining the Risks and Benefits from Benzodiazepines
Rakesh Jain, MD, MPH
Clinical Professor Department of Psychiatry Texas Tech Health Sciences Center School of Medicine Midland, Texas Adjunct Clinical Affiliate University of Texas at Austin School of Nursing Austin, Texas
Saundra Jain, MA, PsyD, LPC
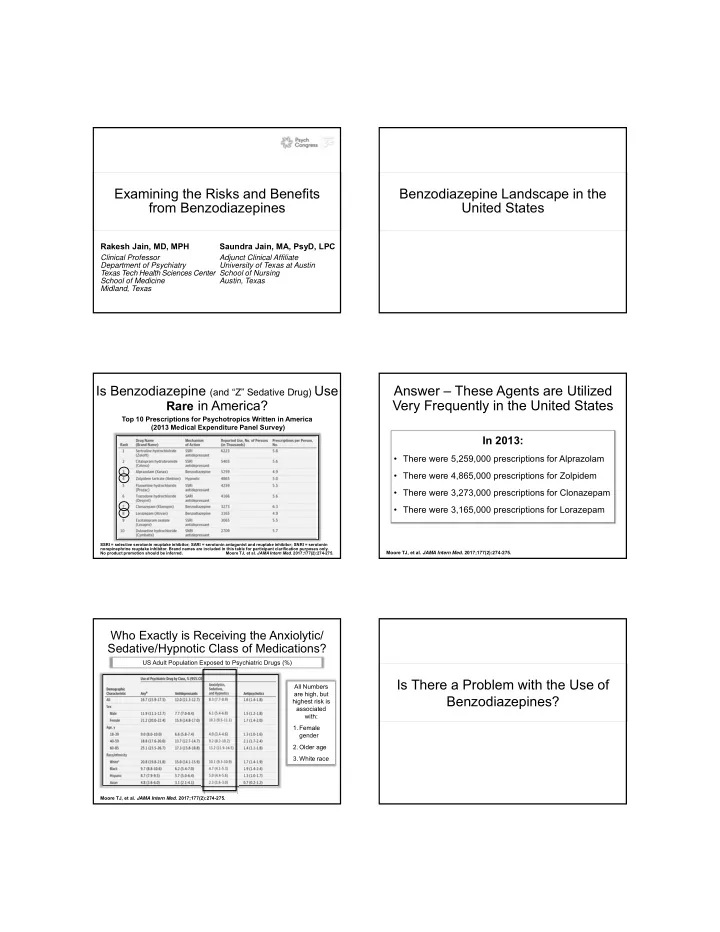
Benzodiazepine Landscape in the United States Is Benzodiazepine (and “Z” Sedative Drug) Use
Rare in America?
SSRI = selective serotonin reuptake inhibitor; SARI = serotonin antagonist and reuptake inhibitor; SNRI = serotonin norepinephrine reuptake inhibitor. Brand names are included in this table for participant clarification purposes only. No product promotion should be inferred. Moore TJ, et al. JAMA Intern Med. 2017;177(2):274-275.
Top 10 Prescriptions for Psychotropics Written in America (2013 Medical Expenditure Panel Survey)
Answer – These Agents are Utilized Very Frequently in the United States
Moore TJ, et al. JAMA Intern Med. 2017;177(2):274-275.
In 2013:
- There were 5,259,000 prescriptions for Alprazolam
- There were 4,865,000 prescriptions for Zolpidem
- There were 3,273,000 prescriptions for Clonazepam
- There were 3,165,000 prescriptions for Lorazepam
Who Exactly is Receiving the Anxiolytic/ Sedative/Hypnotic Class of Medications?
Moore TJ, et al. JAMA Intern Med. 2017;177(2):274-275.
US Adult Population Exposed to Psychiatric Drugs (%) All Numbers are high, but highest risk is associated with:
- 1. Female
gender
- 2. Older age
- 3. White race