SLIDE 1
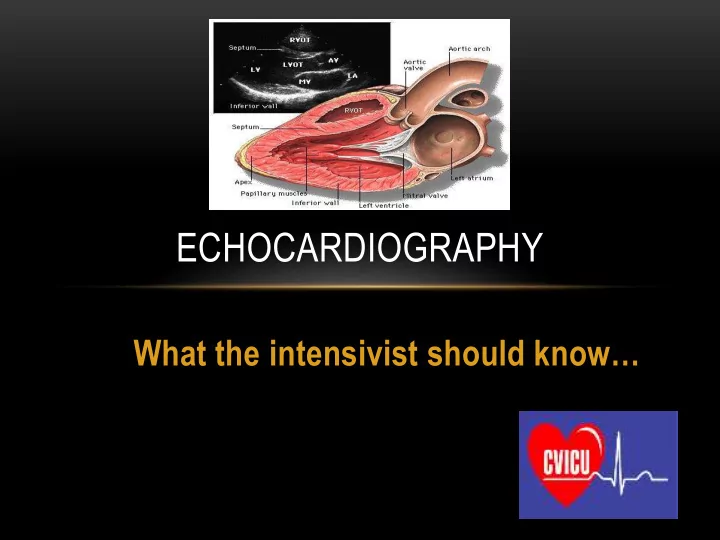
What the intensivist should know…
ECHOCARDIOGRAPHY
SLIDE 2 OVERVIEW
- Background
- Why ECHO?
- Limitations
- How to learn ECHO
- What you need to know
- Where we are heading
SLIDE 3
BACKGROUND
SLIDE 4
SLIDE 5
BACKGROUND
SLIDE 6
COLLEGE AKNOWLEDGEMENT
SLIDE 7 WHY DO WE NEED TO LEARN ECHO?
- Filling the void
- Differentiating shock
- Tamponade post cardiac surgery
- Management of cardiovascular supports
- ECHO in cardiac arrest
SLIDE 8 LIMITATIONS
- Scope of practice
- Impact of
- False positives
- False negatives
- Formal studies
- Advanced studies
SLIDE 9 HOW TO LEARN ECHO
- BOOKS
- COURSES
- WEBSITES
- HANDS ON SACNNING
- SUPERVISION
- POST GRAD CERT/DIPLOMA
SLIDE 10
WEBSITES
SLIDE 11
SLIDE 12 CICM GUIDELINE
- Attend an approved ECHO course
- Find a supervisor
- Perform 35 focussed cardiac ultrasound cases
- Record images/ Write in notes
- Complete and pass an online MCQ exam @CICM
- In the furture- there may be a ‘live’ exam
SLIDE 13 CICM GUIDELINE
- Basic physics
- Machine setup
- Patient details
- Image optimization
- Basic views (PLA/ PSA/ A4C/ Scand IVC)
- Focussed questions looking for pathology
- Limitations
- Colour/Doppler not included
SLIDE 14 CICM GUIDELINE- FOCUSSED QUESTIONS
- 1. Is the LV significantly impaired?
- 2. Is the LV dilated?
- 3. Is the RV function grossly abnormal?
- 4. Is the RV dilated?
- 5. Is there any pericardial fluid/tamponade?
- 6. Is the patient significantly hypovolaemic?
- 7. Conclusion addressing relevant clinical question
SLIDE 15
SLIDE 16
SLIDE 17 SHOCK ALGORITHM
- Assess volume status exclude hypovolaemia
- IVC
- LV EDV
- Assess contractility of LV exclude LV failure
- Exclude tamponade
- Assess right heart function exclude PE
- Exclude pneumothorax
- Exclude AAA
……..takes about 3 minutes….
SLIDE 18 CARDIAC WINDOWS
- Parasternal
- Long axis
- Short Axis
- Apical
- 4 chamber
- 2 chamber
- Subcostal
SLIDE 20
PARASTERNAL LONG AXIS
SLIDE 21
PARASTERNAL LONG AXIS
SLIDE 22
PARSTERNAL SHORT AXIS
SLIDE 23
PARASTERNAL SHORT AXIS
SLIDE 24
PSAX
SLIDE 25
PARASTERNAL SHORT AXIS
SLIDE 26
APICAL 4 CHAMBER
SLIDE 27
APICAL 4 CHAMBER
SLIDE 28
APICAL 4 CHAMBER
SLIDE 29
APICAL 2 CHAMBER
SLIDE 30
APICAL 2 CHAMBER
SLIDE 31
SUBCOSTAL
SLIDE 32
SUBCOSTAL VIEW
SLIDE 33
SUBCOSTAL
SLIDE 34 LV CONTRACTILITY
- Overview
- Visual ‘Gestalt’
- Fractional area change (FAC) (40-60%)
- Simpsons method
- Mild impairment EF 50-70%
- Moderate impairment EF 30-50%
- Severe impairment EF <30%
SLIDE 35
LV CONTRACTILITY- NORMAL
SLIDE 36
LV CONTRACTILITY- NORMAL
SLIDE 37
LV CONTRACTILITY- NORMAL
SLIDE 38
LV CONTRACTILITY- NORMAL
SLIDE 39
LV CONTRACTILITY- NORMAL
SLIDE 40
SLIDE 41
SLIDE 42
SIMPSONS
SLIDE 43
SIMPSONS
SLIDE 44
SLIDE 45
SLIDE 46
SLIDE 47
SLIDE 48
SLIDE 49
SLIDE 50
SLIDE 51
SLIDE 52
SLIDE 53
SLIDE 54
SLIDE 55
SLIDE 56
SLIDE 57
SLIDE 58
SLIDE 59
SLIDE 60
SLIDE 61
SLIDE 62
SLIDE 63
SLIDE 64
SLIDE 65
SLIDE 66
SLIDE 67
SLIDE 68
SLIDE 69
SLIDE 70
SLIDE 71
SLIDE 72
SLIDE 73
SLIDE 74
SLIDE 75
SLIDE 76
SLIDE 77 THE RIGHT VENTRICLE
- Shape
- Size
- Function
- Assesment
SLIDE 78
VOLUME AND PRESSURE OVERLOAD
SLIDE 79
RV/LV RATIO- NORMAL (0.6:1)
SLIDE 80
SLIDE 81 CLASSIC SIGNS OF PE
- Dilated RV
- Septal flattening
- Impaired RV
- Tricuspid regurgitation
- McConnels sign
- Raised PA pressures (RVSP)
- Visible clot
SLIDE 82
SLIDE 83
SLIDE 84
SLIDE 85
SLIDE 86
SLIDE 87
SLIDE 88
SLIDE 89
SLIDE 90
SEPTAL FLATTENING
SLIDE 91
SEPTAL FLATTENING
SLIDE 92
SEPTAL FLATTENING
SLIDE 93 VOLUME STATUS- IVC
- IVC
- Abdominal probe
- Sub-costal view- longitudinal
- Using liver as a window
- Measure IVC 2cm distal to diaphragm
- Collapsibility with respiration
- Visual gestalt
- M-mode
SLIDE 94
IVC DIAMETER AND CVP
SLIDE 95
IVC
SLIDE 96
IVC
SLIDE 97 IVC ANALYSIS
- Absolute diameter
- <1cm Correlates with a CVP ~ <5cm H20
- 1-2cm Correlates with a CVP ~ 5-15cm H20
- >2cm correlates with a CVP ~ >15cm H20
- Variability
- Ventilated patient
- >12% collapsibility indicates volume responsiveness
- Unventilated patient
- >50% collapsibility indicates volume responsiveness
SLIDE 98
VOLUME STATUS-IVC
SLIDE 99
SLIDE 100
SLIDE 101
VOLUME STATUS
SLIDE 102
SLIDE 103
SLIDE 104
SLIDE 105
SLIDE 106
LVEDA NORMAL 12-16 CM
2
SLIDE 107
LVEDA
SLIDE 108
SLIDE 109
SLIDE 110
SLIDE 111
‘KISSING’ PAPILLARY MUSCLES
SLIDE 112
SLIDE 113 PERICARDIAL EFFUSION AND TAMPONADE
- Is there a pericardial effusion/collection?
- <10mm
Small
Moderate
Large
- Is there evidence of tamponade?
- Hypotension
- RA or RV free wall collapse
- Dilated IVC
SLIDE 114
SLIDE 115
SLIDE 116
SLIDE 117
SLIDE 118
SLIDE 119
SLIDE 120
SLIDE 121
SLIDE 122
SLIDE 123
SLIDE 124
SLIDE 125
SLIDE 126
SLIDE 127
SLIDE 128
SLIDE 129
SLIDE 130
SLIDE 131
SLIDE 132
SLIDE 133
SLIDE 134
WHERE THINGS ARE HEADING
SLIDE 135 THE FUTURE
- Portable wireless probes
- Formal basic ECHO training and examinations in CICM
- Advanced ECHO clinician in every ICU
- In-house credentialling and CME
- TOE and disposable probes
SLIDE 136
What the intensivist should know…
ECHOCARDIOGRAPHY