
SLIDE 1
4/14/2016 1
David Rigberg, MD
Professor and Program Director Division of Vascular Surgery University of California Los Angeles
When Do You Need to Treat Venous Perforators?.. and How to Do It
- Disclosures: Speaker honorarium for W.L. Gore
and Associates, 9/2015.
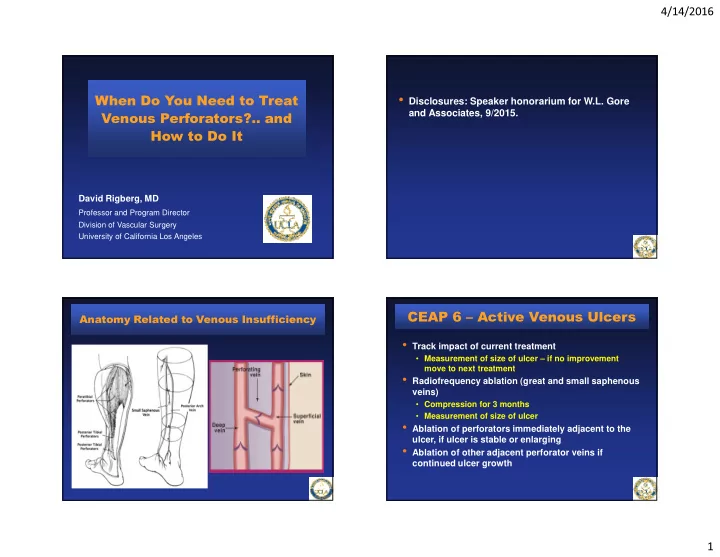
Anatomy Related to Venous Insufficiency
- Track impact of current treatment
- Measurement of size of ulcer – if no improvement
move to next treatment
- Radiofrequency ablation (great and small saphenous
veins)
- Compression for 3 months
- Measurement of size of ulcer
- Ablation of perforators immediately adjacent to the
ulcer, if ulcer is stable or enlarging
- Ablation of other adjacent perforator veins if