
SLIDE 1
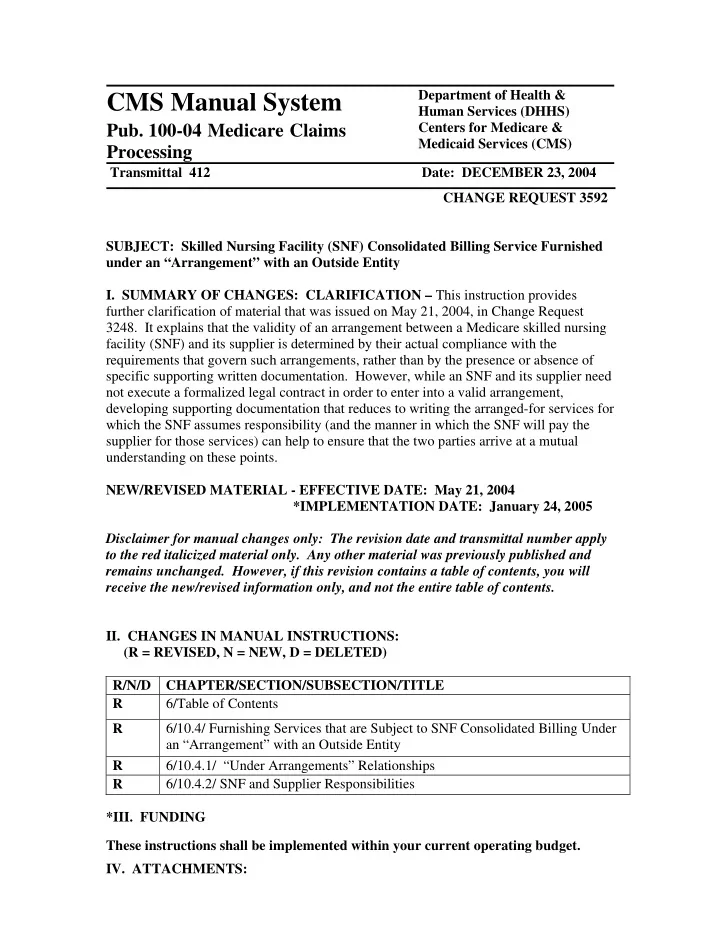
CMS Manual System
Department of Health & Human Services (DHHS)
- Pub. 100-04 Medicare Claims
Processing
Centers for Medicare & Medicaid Services (CMS) Transmittal 412 Date: DECEMBER 23, 2004 CHANGE REQUEST 3592 SUBJECT: Skilled Nursing Facility (SNF) Consolidated Billing Service Furnished under an “Arrangement” with an Outside Entity
- I. SUMMARY OF CHANGES: CLARIFICATION – This instruction provides
further clarification of material that was issued on May 21, 2004, in Change Request
- 3248. It explains that the validity of an arrangement between a Medicare skilled nursing
facility (SNF) and its supplier is determined by their actual compliance with the requirements that govern such arrangements, rather than by the presence or absence of specific supporting written documentation. However, while an SNF and its supplier need not execute a formalized legal contract in order to enter into a valid arrangement, developing supporting documentation that reduces to writing the arranged-for services for which the SNF assumes responsibility (and the manner in which the SNF will pay the supplier for those services) can help to ensure that the two parties arrive at a mutual understanding on these points. NEW/REVISED MATERIAL - EFFECTIVE DATE: May 21, 2004 *IMPLEMENTATION DATE: January 24, 2005 Disclaimer for manual changes only: The revision date and transmittal number apply to the red italicized material only. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents.
- II. CHANGES IN MANUAL INSTRUCTIONS:
(R = REVISED, N = NEW, D = DELETED) R/N/D CHAPTER/SECTION/SUBSECTION/TITLE R 6/Table of Contents R 6/10.4/ Furnishing Services that are Subject to SNF Consolidated Billing Under an “Arrangement” with an Outside Entity R 6/10.4.1/ “Under Arrangements” Relationships R 6/10.4.2/ SNF and Supplier Responsibilities *III. FUNDING These instructions shall be implemented within your current operating budget.
- IV. ATTACHMENTS: