
SLIDE 1
2/9/2017 1
Case Discussion
Michael Wilson, MD, MAS UCSF MS and Neuroinflammation Center
Case
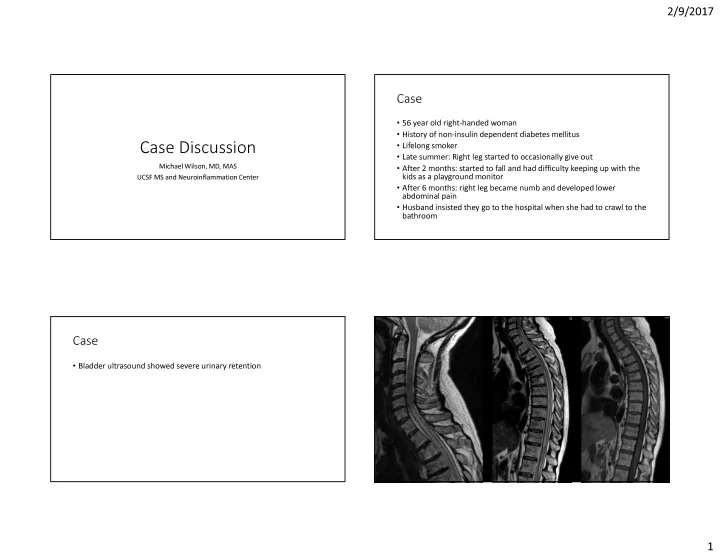
- 56 year old right-handed woman
- History of non-insulin dependent diabetes mellitus
- Lifelong smoker
- Late summer: Right leg started to occasionally give out
- After 2 months: started to fall and had difficulty keeping up with the
kids as a playground monitor
- After 6 months: right leg became numb and developed lower
abdominal pain
- Husband insisted they go to the hospital when she had to crawl to the
bathroom
Case
- Bladder ultrasound showed severe urinary retention