
SLIDE 1
1
Asymptomatic cerebral embolism after AF ablation
Jonathan Kalman Royal Melbourne Hospital No Disclosures
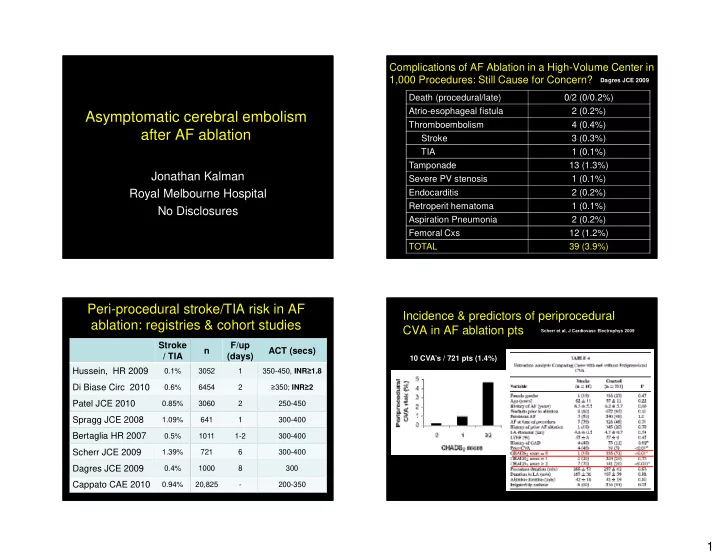
Complications of AF Ablation in a High-Volume Center in 1,000 Procedures: Still Cause for Concern?
Death (procedural/late) 0/2 (0/0.2%) Atrio-esophageal fistula 2 (0.2%) Thromboembolism 4 (0.4%) Stroke 3 (0.3%) TIA 1 (0.1%) Tamponade 13 (1.3%) Severe PV stenosis 1 (0.1%) Endocarditis 2 (0.2%) Retroperit hematoma 1 (0.1%) Aspiration Pneumonia 2 (0.2%) Femoral Cxs 12 (1.2%) TOTAL 39 (3.9%)
Dagres JCE 2009
Peri-procedural stroke/TIA risk in AF ablation: registries & cohort studies
Stroke / TIA n F/up (days) ACT (secs) Hussein, HR 2009
0.1% 3052 1 350-450, INR≥1.8
Di Biase Circ 2010
0.6% 6454 2 ≥350; INR≥2
Patel JCE 2010
0.85% 3060 2 250-450
Spragg JCE 2008
1.09% 641 1 300-400
Bertaglia HR 2007
0.5% 1011 1-2 300-400
Scherr JCE 2009
1.39% 721 6 300-400
Dagres JCE 2009
0.4% 1000 8 300
Cappato CAE 2010
0.94% 20,825
- 200-350
Incidence & predictors of periprocedural CVA in AF ablation pts
Scherr et al, J Cardiovasc Electrophys 2009
10 CVA’s / 721 pts (1.4%)