
SLIDE 1
6/7/2012 1
Integrated Health Service Models for Rural Communities
NOSORH June 7, 2012
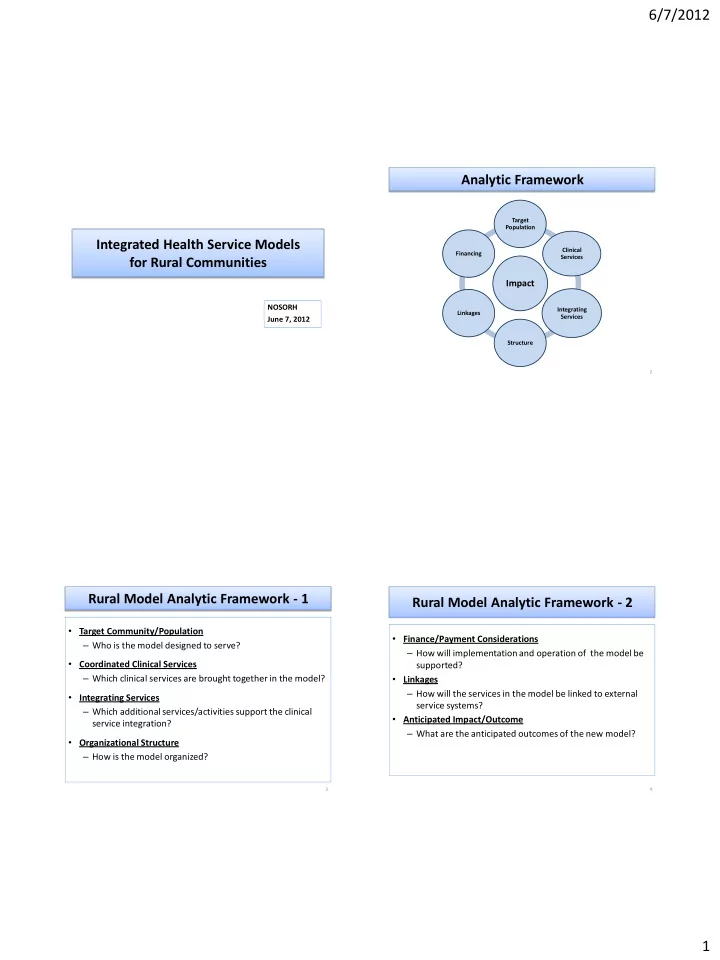
Analytic Framework
Impact
Target Population Clinical Services Integrating Services Structure Linkages Financing
2
Rural Model Analytic Framework - 1
- Target Community/Population
– Who is the model designed to serve?
- Coordinated Clinical Services
– Which clinical services are brought together in the model?
- Integrating Services
– Which additional services/activities support the clinical service integration?
- Organizational Structure
– How is the model organized?
3
Rural Model Analytic Framework - 2
- Finance/Payment Considerations
– How will implementation and operation of the model be supported?
- Linkages
– How will the services in the model be linked to external service systems?
- Anticipated Impact/Outcome
– What are the anticipated outcomes of the new model?
4