
SLIDE 1
3/23/2014 Stage classification % at 5-year survival diagnosis - - PowerPoint PPT Presentation
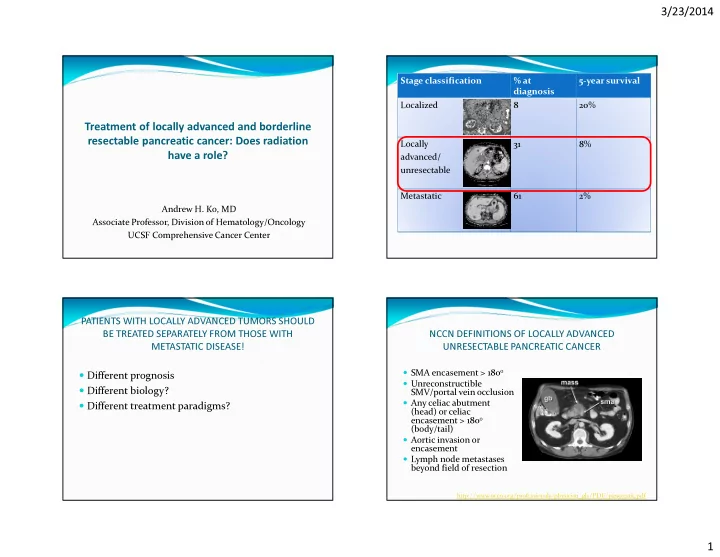
3/23/2014 Stage classification % at 5-year survival diagnosis Localized 8 20% Treatment of locally advanced and borderline resectable pancreatic cancer: Does radiation Locally 31 8% have a role? advanced/ unresectable Metastatic 61
Importance of obtaining
Better symptom palliation
Better likelihood of
Greatest imperative is to
Select out patients who
median surv = 23 weeks
median surv = 42 weeks
median surv = 40 weeks
SMF: median surv = 42 weeks
FU): median surv = 32 weeks
5-FU: median survival = 8.3 mos
mos
Huguet, F. et al. J Clin Oncol; 25:326-331 2007
Huguet, F. et al. J Clin Oncol; 25:326-331 2007
Median PFS 10.8 vs. 7.4 mos (p=0.005) Median OS 15.0 vs. 11.7 mos (p=0.0009)
Induction chemotherapy Gemcitabine x 4 months Gemcitabine x 2 months Stop until progression RT (5400 cGy) + capecitabine Stop until progression Gemcitabine plus erlotinib x 4 months Gemcitabine plus erlotinib x 2 months Erlotinib until progression RT (5400 cGy) + capecitabine Erlotinib until progression
Borderline resectable disease E N R O L L FOLFIRINOX 4 cycles + 2 - 6 weeks break R E S T A G E R E S T A G E SURGERY + 6 – 8 weeks break R E S T A G E 50.4g EBRT + CAPE + 4 – 10 weeks break F O L L O W GEM 2 x 28 day cycle
6.6 Gy x 5
Enteritis
Fistula (1), ulcer (3)
Up-front chemoRT has produced mixed results Growing interest in delayed chemoRT, although recent LAP-07 trial raises
Selection of radiosensitizing agents Radiation techniques and dosing Predictive biomarkers (e.g. DPC4)
Again, role of neoadjuvant RT in this context has yet to be defined