
SLIDE 1
2/14/2014 1 Disclosures
- NIH- U01 NS062835 (Co-PI) POINT
- DMCs for Daiichi-Sankyo, Schering-
Plough Research Institute and Novartis
- Advisory Board for AstraZeneca
- J. Donald Easton, MD
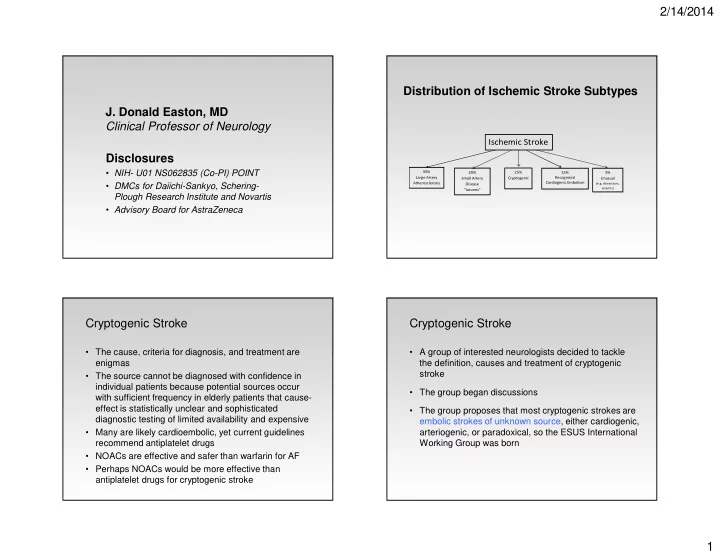
Clinical Professor of Neurology Distribution of Ischemic Stroke Subtypes
Ischemic Stroke
35% Large Artery Atherosclerosis 20% Small Artery Disease “lacunes” 15% Recognized Cardiogenic Embolism 5% Unusual
(e.g. dissections, arteritis)
25% Cryptogenic
Cryptogenic Stroke
- The cause, criteria for diagnosis, and treatment are
enigmas
- The source cannot be diagnosed with confidence in
individual patients because potential sources occur with sufficient frequency in elderly patients that cause- effect is statistically unclear and sophisticated diagnostic testing of limited availability and expensive
- Many are likely cardioembolic, yet current guidelines
recommend antiplatelet drugs
- NOACs are effective and safer than warfarin for AF
- Perhaps NOACs would be more effective than
antiplatelet drugs for cryptogenic stroke
Cryptogenic Stroke
- A group of interested neurologists decided to tackle
the definition, causes and treatment of cryptogenic stroke
- The group began discussions
- The group proposes that most cryptogenic strokes are