
NATIONAL COMMISSION FOR GOVERNMENT REFORMS
Recommendations of the Sub-Committee on Health
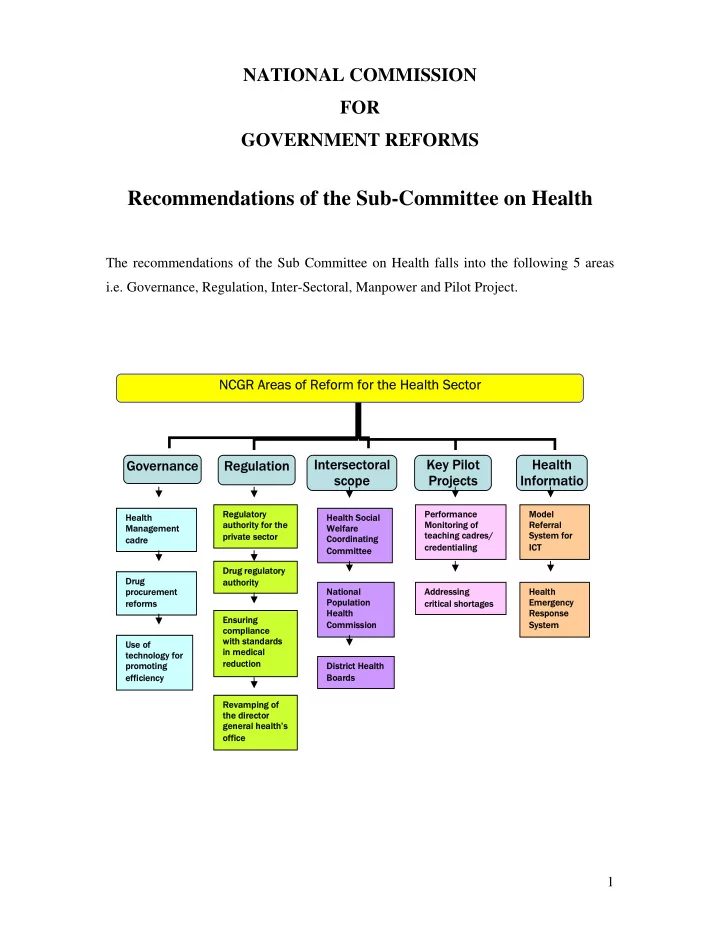
The recommendations of the Sub Committee on Health falls into the following 5 areas i.e. Governance, Regulation, Inter-Sectoral, Manpower and Pilot Project. NCGR Areas of Reform for the Health Sector NCGR Areas of Reform for the Health Sector Inte tersecto rsectoral ral scope scope Key Pilo Key Pilot t Projects Projects Hea Health th Informat Informatio io Gove Governa rnance nce Regulation Regulation 1
Regu Regulatory tory auth author
- rity for
ity for the the pri private ate s sect ctor Performa Performance nce Moni Monito tori ring o ng of teac teaching cad hing cadres/ es/ crede credentia tialing ing Mo Mode del Referral Referral Sy System for stem for ICT ICT Heal Health th So Soci cial al Welfare Welfare Co Coor
- rdin
dinating Comm mmittee ittee Drug re ug regulat gulatory ry auth author
- rity
ity Dr Drug procurement procurement ref reform rms Nati National al Po Populati tion
- n
Heal Health th Co Comm mmissi ssion Addre Addressing ng cr crit itica ical sh shortage
- rtages
s Heal Health th Emer Emergency gency Resp spon
- nse
se Sy System stem Ens Ensuring ng co compli liance wi with s standards in med in medical cal reduct reduction ion Us Use o e of tec technology f nology for promot
- moting
ing eff efficiency ency Dis Distri rict H Heal alth Bo Boards ds Heal Health th Manage Management ment cadre cadre Revamp Revamping o g of the the director director gene general hea ral health’ th’s
- f
- ffi
fice ce