
1
International Liver Congress 2019: Update from Vienna
Jordan J. Feld MD MPH
Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto
Disclosures
- Dr. Feld
- Research: Abbott, Abbvie, Gilead, Janssen, Merck
- Consulting: Abbvie, Gilead, Merck
Dr Shah
- Consulting Fees: Abbvie, Gilead, Merck, Intercept, Lupin
Learning Objectives
- 1. Appreciate recent advances in HBV and HCV presented at the
International Liver Congress 2019
- 2. Put into context the recent Phase 3 trial results for a new therapy
for NASH
Outline
- HCV
– Screening & linkage to care – Treatment efficacy – Treatment monitoring – HCC post-SVR
- HBV
– Current therapies
- Cancer risk
- Transmission risk
- NASH
– Obeticholic acid for NASH – REGENERATE Trial
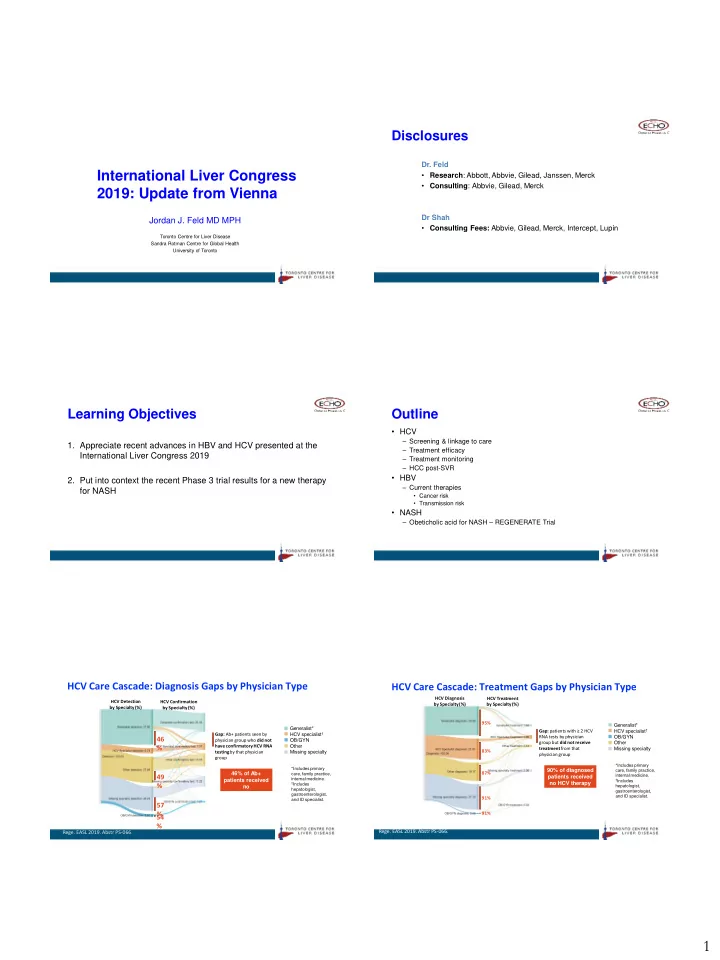
HCV Care Cascade: Diagnosis Gaps by Physician Type
46 % 49 % 57 % 54 %
Gap: Ab+ patients seen by physician group who did not have confirmatory HCV RNA testing by that physician group HCV Detection by Specialty (%) HCV Confirmation by Specialty (%) Generalist* HCV specialist† OB/GYN Other Missing specialty *Includes primary care, family practice, internal medicine.
†Includes
hepatologist, gastroenterologist, and ID specialist.
46% of Ab+ patients received no HCV RNA test
- Rege. EASL 2019. Abstr PS-066.
HCV Diagnosis by Specialty (%) HCV Treatment by Specialty (%) Generalist* HCV specialist† OB/GYN Other Missing specialty *Includes primary care, family practice, internal medicine.
†Includes
hepatologist, gastroenterologist, and ID specialist.
90% of diagnosed patients received no HCV therapy
- Rege. EASL 2019. Abstr PS-066.
Gap: patients with ≥ 2 HCV RNA tests by physician group but did not receive treatment from that physician group 95% 83% 91% 87% 91%