
SLIDE 1
1
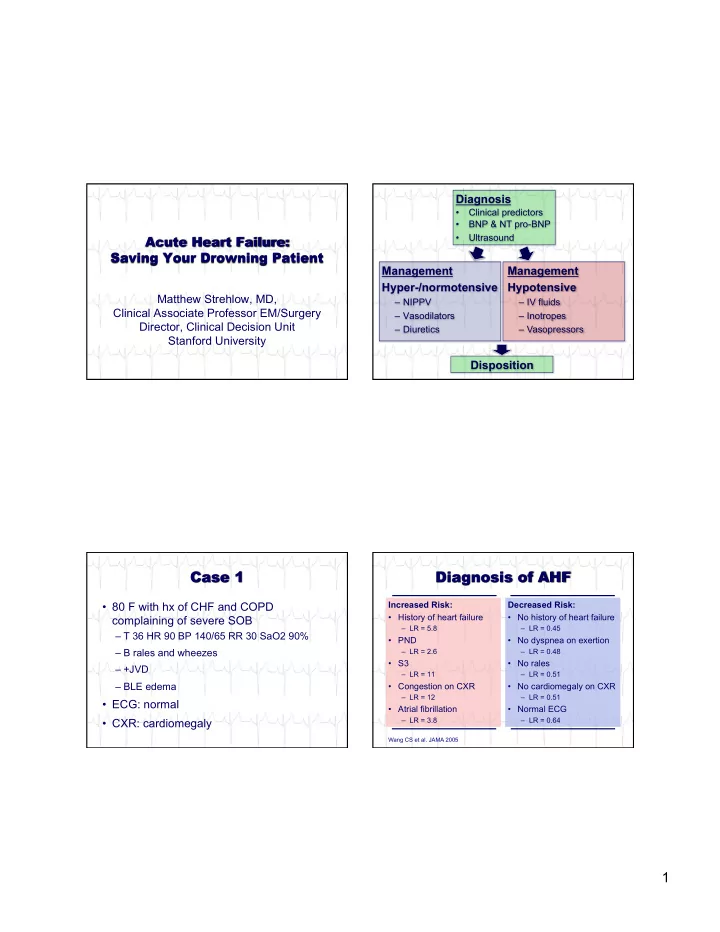
Matthew Strehlow, MD, Clinical Associate Professor EM/Surgery Director, Clinical Decision Unit Stanford University Management Hyper-/normotensive
– NIPPV – Vasodilators – Diuretics
Management Hypotensive
– IV fluids – Inotropes – Vasopressors
Diagnosis
- Clinical predictors
- BNP & NT pro-BNP
- Ultrasound
Disposition
- 80 F with hx of CHF and COPD
complaining of severe SOB
– T 36 HR 90 BP 140/65 RR 30 SaO2 90% – B rales and wheezes – +JVD – BLE edema
- ECG: normal
- CXR: cardiomegaly
Decreased Risk:
- No history of heart failure
– LR = 0.45
- No dyspnea on exertion
– LR = 0.48
- No rales
– LR = 0.51
- No cardiomegaly on CXR
– LR = 0.51
- Normal ECG
– LR = 0.64
Increased Risk:
- History of heart failure
– LR = 5.8
- PND
– LR = 2.6
- S3
– LR = 11
- Congestion on CXR
– LR = 12
- Atrial fibrillation
– LR = 3.8
Wang CS et al. JAMA 2005