
SLIDE 1
1
Management of Heart Failure with Reduced Ejection Fraction
What Does the Evidence Show Us?
James C. Fang, MD University of Utah Health Sciences Salt Lake City, UT
65 yr WM presents for followup of HFrEF.
– NYHA II-III, HFH 6 mo ago. Prior CABG, DM and HTN. LVEF 30%. – Meds: lisinopril 10 mg, carvedilol 12.5 mg bid, spironolactone 25 mg, furosemide 40 mg, metformin 500 mg, aspirin, atorvastatin 40 mg. – BP 122/75, HR 73, BMI 28, NAD, no JVD, HS normal, sternal scar, lungs clear, no edema. – EKG SR anterior Qs, NT-proBNP 1500, Cr 1.2, Hgb A1c 8.2%.
What Next?
- A. No changes
- B. Ivabradine
- C. Sacubitril/valsartan
- D. Empagliflozin
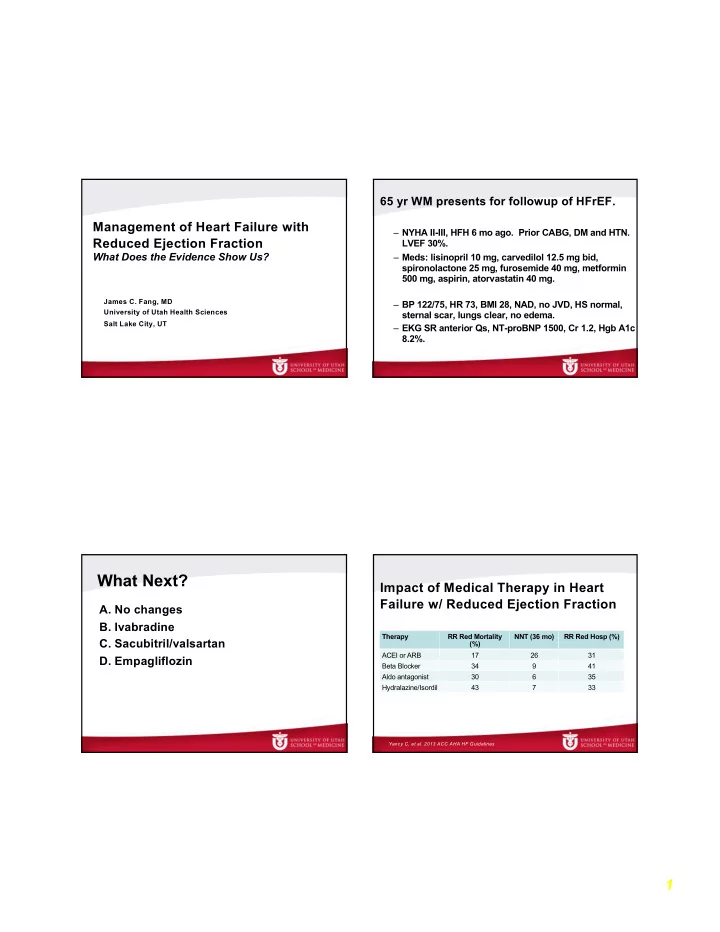
Impact of Medical Therapy in Heart Failure w/ Reduced Ejection Fraction
Therapy RR Red Mortality (%) NNT (36 mo) RR Red Hosp (%) ACEI or ARB 17 26 31 Beta Blocker 34 9 41 Aldo antagonist 30 6 35 Hydralazine/Isordil 43 7 33
Yancy C, et al. 2013 ACC AHA HF Guidelines