
SLIDE 1
1/31/2020 1
Upstream Priority:
the role of social determinants in promoting health
Greg Moody, Executive in Residence moody.67@osu.edu February 3, 2020
JOHN GLENN COLLEGE OF PUBLIC AFFAIRS
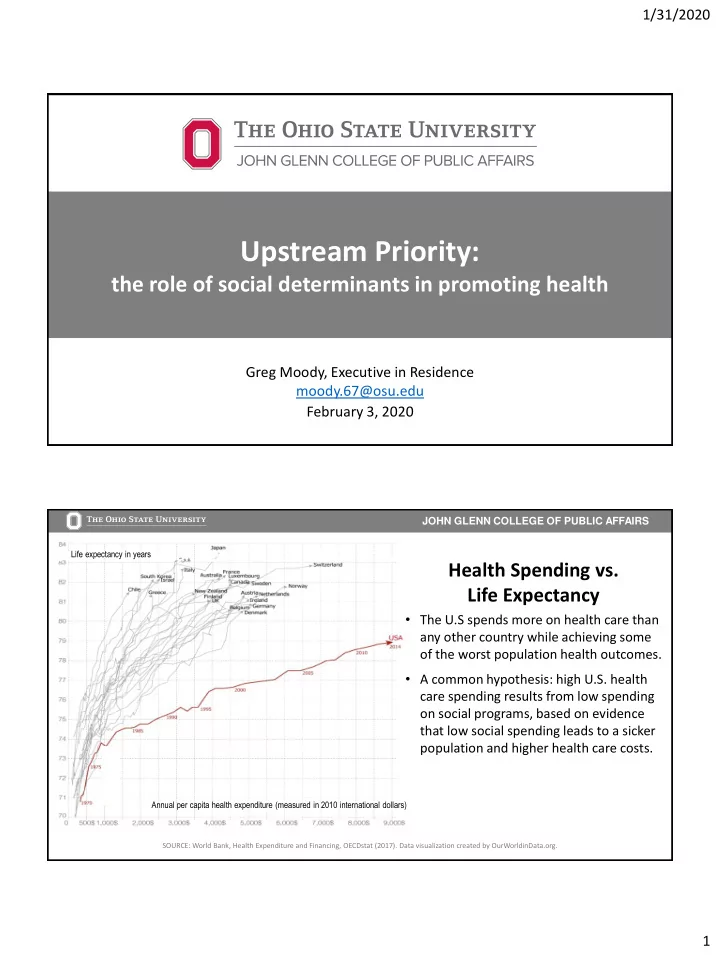
SOURCE: World Bank, Health Expenditure and Financing, OECDstat (2017). Data visualization created by OurWorldinData.org.
Health Spending vs. Life Expectancy
- The U.S spends more on health care than
any other country while achieving some
- f the worst population health outcomes.
- A common hypothesis: high U.S. health
care spending results from low spending
- n social programs, based on evidence
that low social spending leads to a sicker population and higher health care costs.
Annual per capita health expenditure (measured in 2010 international dollars) Life expectancy in years