
SLIDE 1
1
No Disclosures
Tricuspid Regurgitation:
Implication for Left-sided Procedures
Chari Y.T. Hart MD, FACC
Interventional Echocardiography
Queen’s Heart Physician Practice Queen’s Medical Center-Honolulu, Hawaii Assistant Clinical Professor of Medicine, John A. Burns School of Medicine, University of Hawaii
October 01, 2016
Innovative Procedures, Devices, and State of the Art Care for Arrhythmias, Heart Failure and Structural Heart Disease
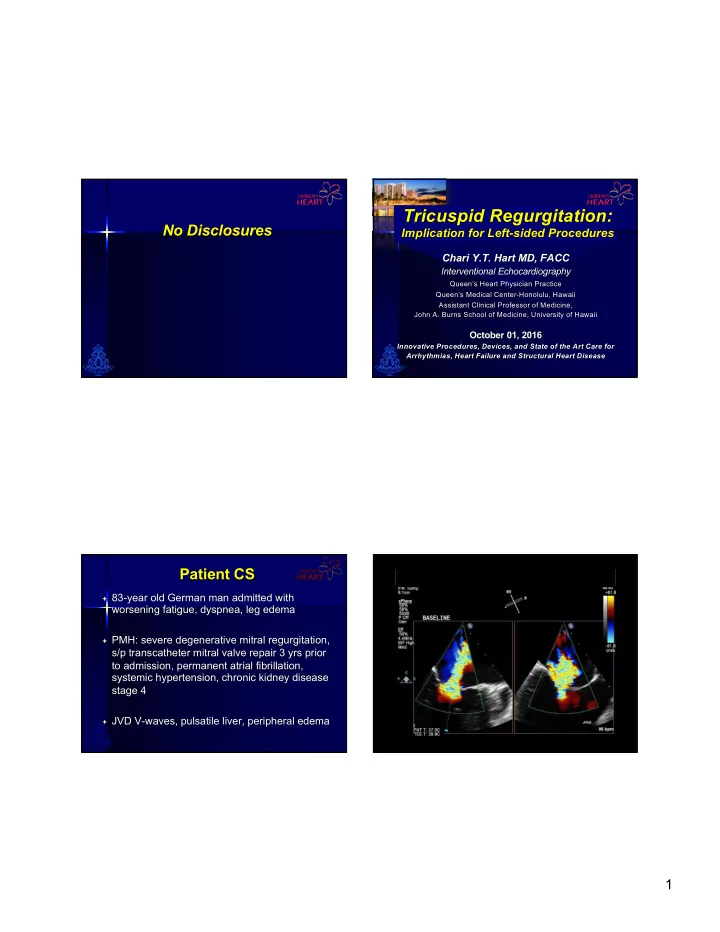
Patient CS
ª 83-year old German man admitted with
worsening fatigue, dyspnea, leg edema
ª PMH: severe degenerative mitral regurgitation,
s/p transcatheter mitral valve repair 3 yrs prior to admission, permanent atrial fibrillation, systemic hypertension, chronic kidney disease stage 4
ª JVD V-waves, pulsatile liver, peripheral edema