
SLIDE 1
8/5/2013 1
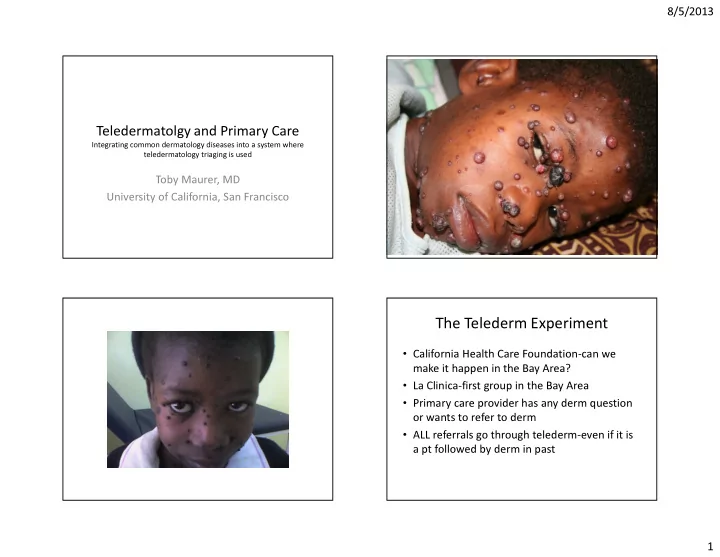
Teledermatolgy and Primary Care
Integrating common dermatology diseases into a system where teledermatology triaging is used
Toby Maurer, MD University of California, San Francisco
The Telederm Experiment
- California Health Care Foundation-can we
make it happen in the Bay Area?
- La Clinica-first group in the Bay Area
- Primary care provider has any derm question
- r wants to refer to derm
- ALL referrals go through telederm-even if it is