
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS] 3/7/2015 1
The surgical management of medullary thyroid cancer
Updated guidelines
3/6/15
Jessica E. Gosnell MD Associate Professor of Clinical Surgery
3/6/15 Surgical management of MTC 2
Nothing to disclose
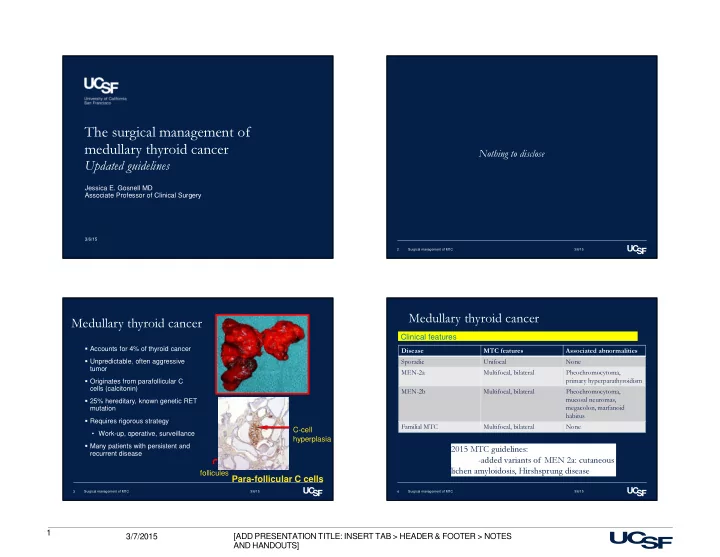
Medullary thyroid cancer
Accounts for 4% of thyroid cancer Unpredictable, often aggressive tumor Originates from parafollicular C cells (calcitonin) 25% hereditary, known genetic RET mutation Requires rigorous strategy
- Work-up, operative, surveillance
Many patients with persistent and recurrent disease
3/6/15 Surgical management of MTC 3
Para-follicular C cells
follicules C-cell hyperplasia
Medullary thyroid cancer
Disease MTC features Associated abnormalities Sporadic Unifocal None MEN-2a Multifocal, bilateral Pheochromocytoma, primary hyperparathyroidism MEN-2b Multifocal, bilateral Pheochromocytoma, mucosal neuromas, megacolon, marfanoid habitus Familial MTC Multifocal, bilateral None
Clinical features
3/6/15 Surgical management of MTC 4
2015 MTC guidelines:
- added variants of MEN 2a: cutaneous