
SLIDE 1
5/30/2013 1
Transfusion Ratios: What’s the Evidence?
Rachael Callcut, MD, MSPH Assistant Professor of Surgery, UCSF
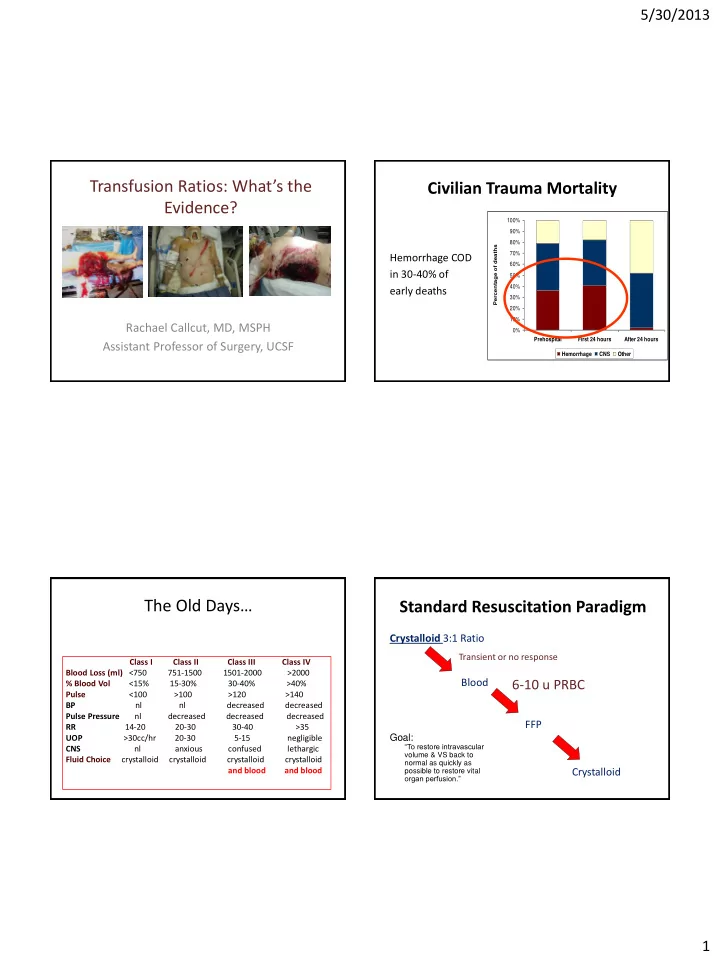
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Prehospital First 24 hours After 24 hours Percentage of deaths Hemorrhage CNS Other Data adapted from: Acosta, et al. J Am Coll Surg 1998 & Sauaia, et al. J Trauma 1995
Civilian Trauma Mortality
Hemorrhage COD in 30-40% of early deaths
The Old Days…
Class I Class II Class III Class IV Blood Loss (ml) <750 751-1500 1501-2000 >2000 % Blood Vol <15% 15-30% 30-40% >40% Pulse <100 >100 >120 >140 BP nl nl decreased decreased Pulse Pressure nl decreased decreased decreased RR 14-20 20-30 30-40 >35 UOP >30cc/hr 20-30 5-15 negligible CNS nl anxious confused lethargic Fluid Choice crystalloid crystalloid crystalloid crystalloid and blood and blood
Standard Resuscitation Paradigm
Crystalloid 3:1 Ratio Blood FFP
Transient or no response
6-10 u PRBC
Crystalloid
Goal:
“To restore intravascular volume & VS back to normal as quickly as possible to restore vital
- rgan perfusion.”