
SLIDE 1
1
Endpoints of Resuscitation for Endpoints of Resuscitation for Circulatory Shock: Circulatory Shock: When Enough is Enough? When Enough is Enough?
Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital Detroit, Michigan erivers1@hfhs.org
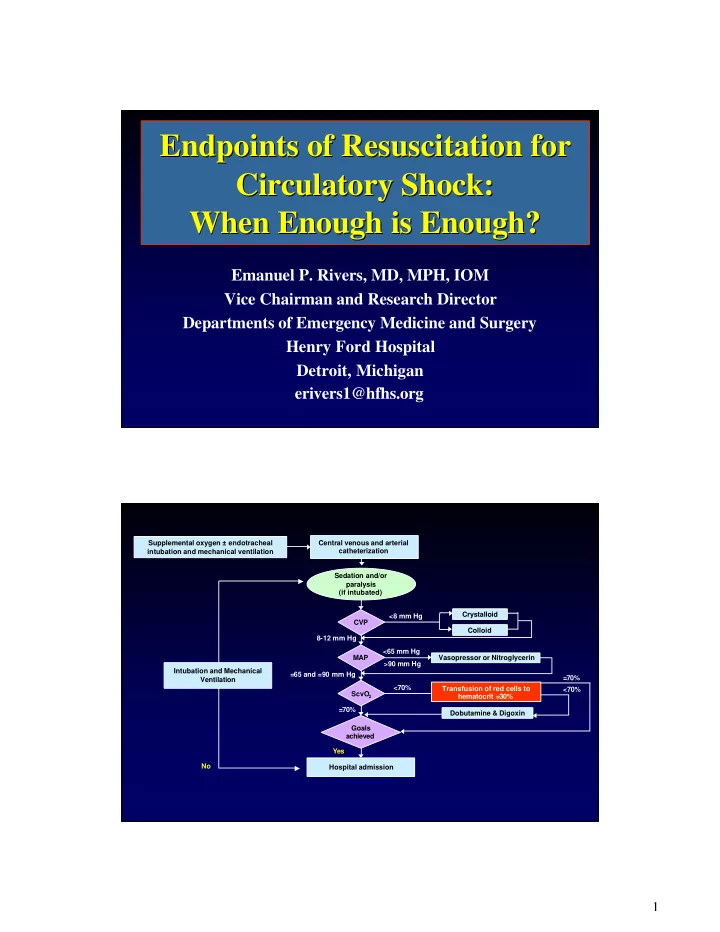
Supplemental oxygen ± endotracheal intubation and mechanical ventilation Central venous and arterial catheterization CVP Crystalloid Colloid <8 mm Hg MAP 8-12 mm Hg Vasopressor or Nitroglycerin <65 mm Hg >90 mm Hg ScvO
2
=65 and =90 mm Hg Goals achieved =70% Hospital admission Yes No Sedation and/or paralysis (if intubated) Transfusion of red cells to hematocrit =30% <70% Dobutamine & Digoxin <70% =70% Intubation and Mechanical Ventilation