
SLIDE 1
4/6/2017 1
William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles, California
Intramural Hematoma (IMH) Should we treat this aggressively?
Disclosures
- Speaker / consultant
W.L. Gore Endologix Medtronic
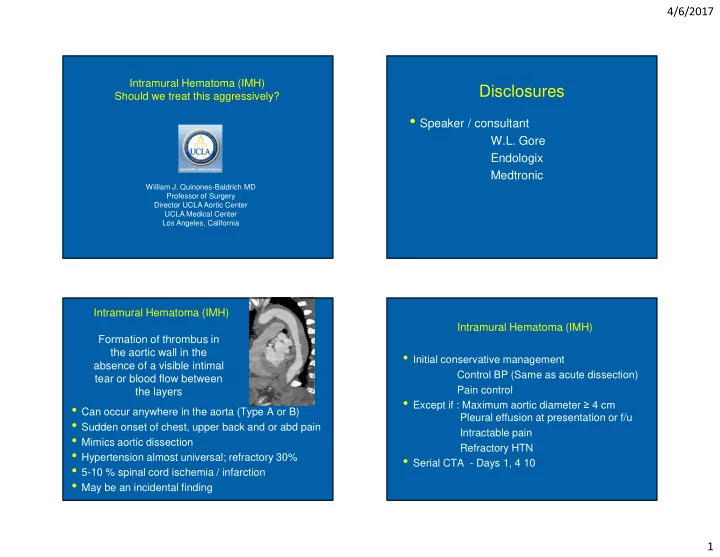
Formation of thrombus in the aortic wall in the absence of a visible intimal tear or blood flow between the layers
- Can occur anywhere in the aorta (Type A or B)
- Sudden onset of chest, upper back and or abd pain
- Mimics aortic dissection
- Hypertension almost universal; refractory 30%
- 5-10 % spinal cord ischemia / infarction
- May be an incidental finding
Intramural Hematoma (IMH)
- Initial conservative management
Control BP (Same as acute dissection) Pain control
- Except if : Maximum aortic diameter ≥ 4 cm
Pleural effusion at presentation or f/u Intractable pain Refractory HTN
- Serial CTA - Days 1, 4 10