
SLIDE 1
7/23/2013 1
Common Knee Problems: What You “Knee’d” to Know
UCSF Essentials of Primary Care August 8, 2013 Carlin Senter, M.D.
Learning objectives: in 50 minutes you will be able to…
- 1. List the organizational scheme for any
musculoskeletal work‐up
- 2. List the 3 key knee history questions
- 3. Generate a differential diagnosis for acute knee
injury with effusion
- 4. Generate a differential diagnosis for chronic
anterior knee pain
- 5. Treat a patient with knee OA and meniscus tear
- 6. QUIZ
Musculoskeletal work‐up
- History
- Inspection
- Palpation
- Range of motion
- Other Tests
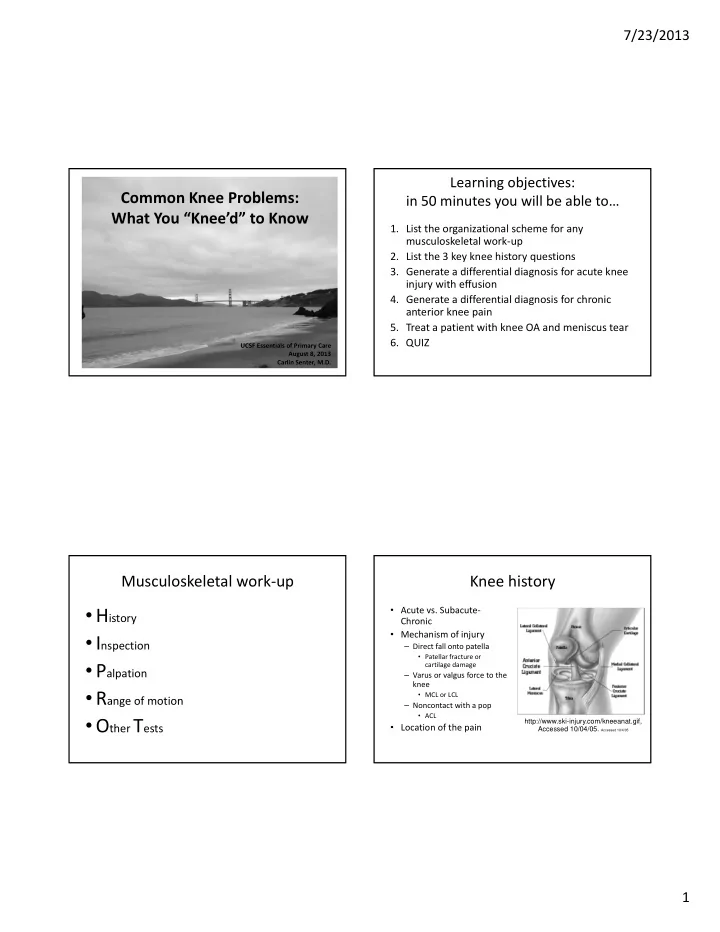
Knee history
- Acute vs. Subacute‐
Chronic
- Mechanism of injury
– Direct fall onto patella
- Patellar fracture or
cartilage damage
– Varus or valgus force to the knee
- MCL or LCL
– Noncontact with a pop
- ACL
- Location of the pain
http://www.ski-injury.com/kneeanat.gif, Accessed 10/04/05. Accessed 10/4/05