
SLIDE 1
10/1/2018 1
Rheumatoid Arthritis in Asians
Mary C. Nakamura M.D. Professor of Medicine, UCSF
NO DISCLOSURES
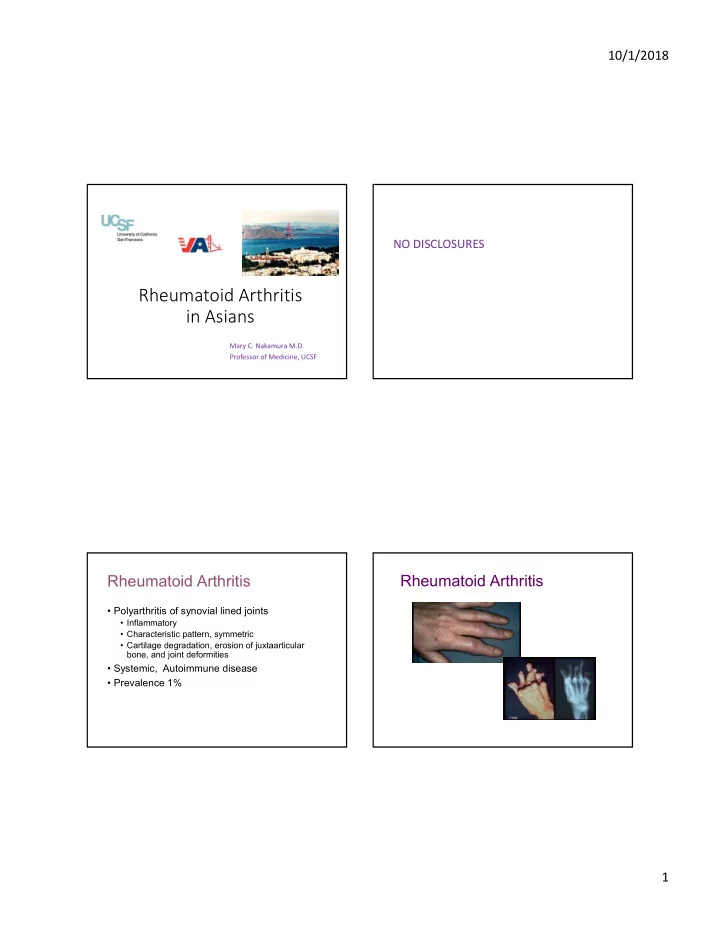
Rheumatoid Arthritis
- Polyarthritis of synovial lined joints
- Inflammatory
- Characteristic pattern, symmetric
- Cartilage degradation, erosion of juxtaarticular
bone, and joint deformities
- Systemic, Autoimmune disease
- Prevalence 1%