
SLIDE 1
1
Psoriasis
Mark A. Bechtel, M.D.
Director of Dermatology The Ohio State University College of Medicine
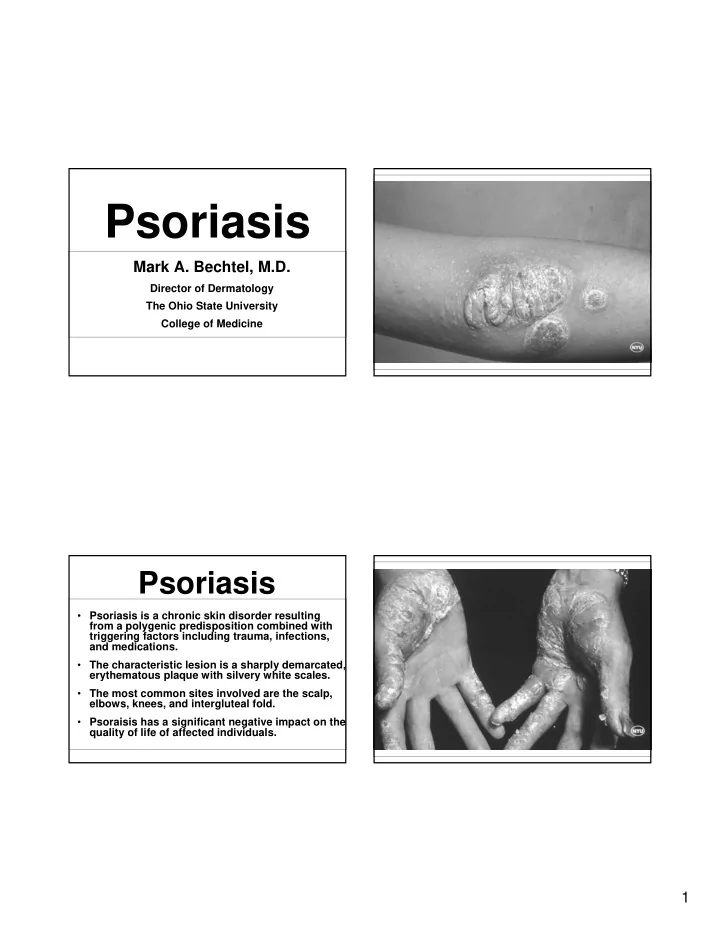
Psoriasis
- Psoriasis is a chronic skin disorder resulting
from a polygenic predisposition combined with triggering factors including trauma, infections, and medications.
- The characteristic lesion is a sharply demarcated,
erythematous plaque with silvery white scales.
- The most common sites involved are the scalp,
elbows, knees, and intergluteal fold.
- Psoraisis has a significant negative impact on the
quality of life of affected individuals.