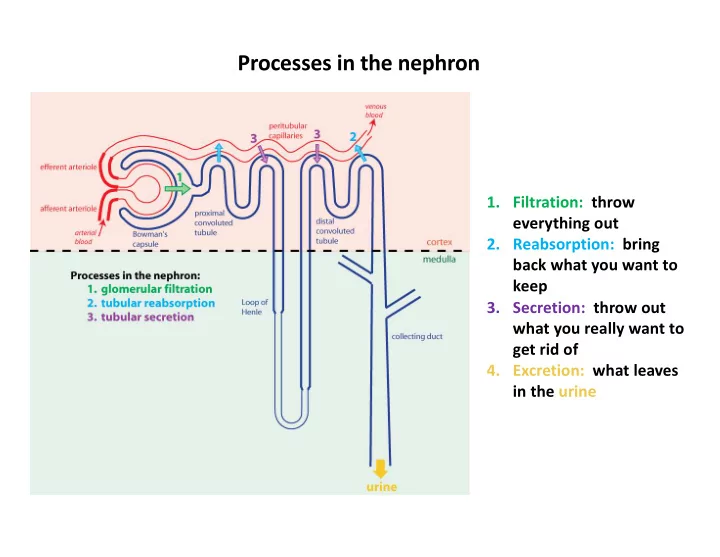
SLIDE 1 Processes in the nephron
everything out
back what you want to keep
what you really want to get rid of
- 4. Excretion: what leaves
in the urine
SLIDE 2 Water balance involves the homeostatic regulation
SLIDE 3 Osmosis and osmotic pressure
Figure 5.2
SLIDE 4
Water reabsorption involves the loops of Henle and the collecting ducts in the medulla
SLIDE 5
Formation of osmotic gradient by the loop of Henle
NOTE: don’t worry about details; just know that the loop of Henle is the part of the nephron responsible for generating the osmotic gradient
SLIDE 6
Regulated water permeability in the collecting duct
SLIDE 7 Vasopressin
- also known as antidiuretic hormone (ADH)
- hormone released at the posterior pituitary
- released by neurosecretory cells
- hormone release regulated by osmoreceptors located in
hypothalamus
SLIDE 8 Neurosecretory cell
- neurosecretory cells have their cell bodies located in the hypothalamus
SLIDE 9
Vander’s Physiology 12th edition, Fig. 11-13a
Hypothalamus and pituitary
SLIDE 10
Neurosecretory cells of the hypothalamus
anterior pituitary posterior pituitary Vander’s Physiology 12th edition, Fig. 11-13b
SLIDE 11
Vasopressin regulates water permeability by increasing aquaporins (AQP2) in the apical plasma membrane of the collecting duct
SLIDE 12
Collecting duct
collecting ducts near papilla the collecting duct is lined with a crisp, clear, cuboidal epithelium
SLIDE 13
Patient D
What is the term for excessive urine production? Why does hyperglycemia in diabetes mellitus cause increased urine production? What sensors are responsible for promoting thirst?
SLIDE 14
Saturation of sodium-glucose cotransporters in the kidney tubules leads to polyuria
SLIDE 15
SLIDE 16
Patient D: Test Results
SLIDE 17
Osmolarity: solute/liter of water Osmolality: solute/kilogram of water
SLIDE 18
Diabetes insipidus: polyuria due to a defect in the ability to reabsorb water and concentrate urine
central diabetes insipidus: deficiency of vasopressin nephrogenic diabetes insipidus: kidney doesnt respond to vasopressin
SLIDE 19
What type of cell releases vasopressin? Where are the cell bodies of vasopressin-secreting cells located? What sensors regulate vasopressin release, and where are they located?
SLIDE 20
Patient D
Diagnosis: adipsic diabetes insipidus due to tumor in the hypothalamus Treatment: vasopressin agonist; guidelines for fluid intake
SLIDE 21
Patient E
What does a diuretic do? What specific part of the nephron is damaged to cause proteinuria?
SLIDE 22 Filtration Occurs in the Renal Corpuscle
Figure 19.5
SLIDE 23 Filtration membrane
Figure 19.5c, d; p.596 schematic of a cross-section through two capillary loops
schematic cross-section through filtration membrane, highly magnified
SLIDE 24 Proteinuria: sign of damage to the filtration membrane
Barriers to filtration of protein:
- 1. negative charge in glycocalyx
- 2. meshwork of proteins in
glomerular basement membrane
- 3. meshwork of proteins in the slit
diaphragm
SLIDE 25
serum creatinine
metabolism of creatine from skeletal muscle excretion in the urine Does the patient’s increasing serum creatinine indicated that her kidney function is deteriorating or improving?
SLIDE 26 Diabetic Nephropathy
- leading cause of end-stage renal disease (end stage renal disease is
kidney function so low it requires renal replacement: either dialysis or kidney transplant)
- hyperglycemia and/or decreased insulin signaling cause changes to
the glomerulus to cause leaky filtration barrier and proteinuria
- proteinuria damages nephrons and leads to nephron loss
SLIDE 27
Incidence of ESRD by primary diagnosis
From US Renal Data System 2014 Report http://www.usrds.org/2014/view/Default.aspx
Data from 1980-2012 Data from 1996-2014
From US Renal Data System 2016 Report http://www.usrds.org/2016/view/Default.aspx
SLIDE 28 Glomerular filtration rate (GFR)
- rate of fluid flow into Bowman’s space
- important measure of kidney function
SLIDE 29
Renal Clearance
SLIDE 30 Processes in the nephron
everything out
back what you want to keep
what you really want to get rid of
- 4. Excretion: what leaves
in the urine
SLIDE 31 Inulin
- don’t confuse with insulin
- plant carbohydrate (must be injected)
- freely filtered
- neither reabsorbed nor secreted
SLIDE 32
SLIDE 33
SLIDE 34
SLIDE 35 Filtered Load
- filtered load = amount filtered
- filtration: bulk flow of plasma and
all small substances dissolved in it
SLIDE 36