
SLIDE 1
10/15/2015 1
Prenatal Aneuploidy Screening Using cell Free DNA
Mary E. Norton MD Professor, Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco
What Does the Evidence Tell Us? Oct 2015
Disclosures
- Research support from Natera and Ariosa
- No lucrative personal financial contracts
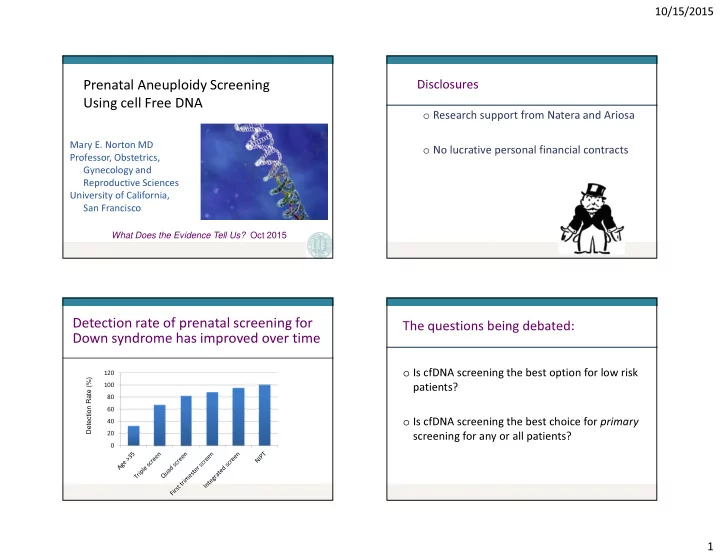
20 40 60 80 100 120
Detection rate of prenatal screening for Down syndrome has improved over time
Detection Rate (%)
The questions being debated:
- Is cfDNA screening the best option for low risk
patients?
- Is cfDNA screening the best choice for primary