
SLIDE 1
Physical Examination of the Respiratory System
Observation and Inspection If a patient presents with specific symptoms, you’re able to tailor your history taking and physical exam to focus on specific organ systems. So what are some symptoms that might point to a respiratory problem?
- 1. Runny, blocked nose and sneezing
- 2. Cough
- 3. Chest pain
- 4. Shortness of breath (dyspnea)
- 5. Wheezing
- 6. Swollen feet/ankles (peripheral edema)
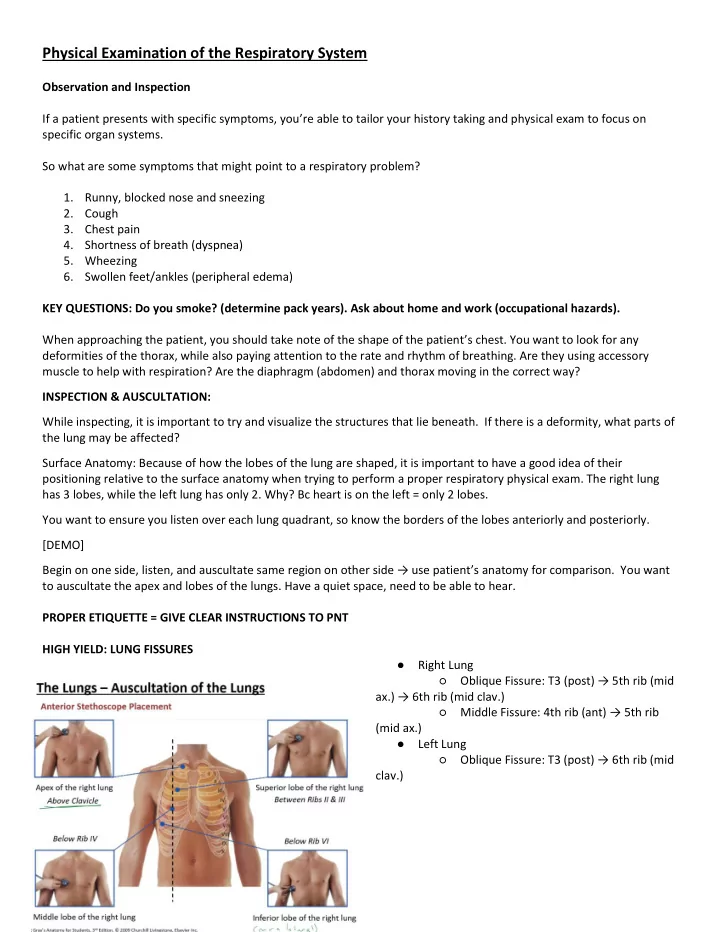
KEY QUESTIONS: Do you smoke? (determine pack years). Ask about home and work (occupational hazards). When approaching the patient, you should take note of the shape of the patient’s chest. You want to look for any deformities of the thorax, while also paying attention to the rate and rhythm of breathing. Are they using accessory muscle to help with respiration? Are the diaphragm (abdomen) and thorax moving in the correct way? INSPECTION & AUSCULTATION: While inspecting, it is important to try and visualize the structures that lie beneath. If there is a deformity, what parts of the lung may be affected? Surface Anatomy: Because of how the lobes of the lung are shaped, it is important to have a good idea of their positioning relative to the surface anatomy when trying to perform a proper respiratory physical exam. The right lung has 3 lobes, while the left lung has only 2. Why? Bc heart is on the left = only 2 lobes. You want to ensure you listen over each lung quadrant, so know the borders of the lobes anteriorly and posteriorly. [DEMO] Begin on one side, listen, and auscultate same region on othe side → use patiet’s anatomy for comparison. You want to auscultate the apex and lobes of the lungs. Have a quiet space, need to be able to hear. PROPER ETIQUETTE = GIVE CLEAR INSTRUCTIONS TO PNT HIGH YIELD: LUNG FISSURES
- Right Lung
○ Oblique Fissure: T post → th i id
- a. → th i id lav.
○ Middle Fissue: th i at → th i (mid ax.)
- Left Lung