
SLIDE 1
21/04/2018
PAH related to congenital heart disease in the adult
Kostas Dimopoulos MD MSc PhD FESC Adult Congenital Heart Centre & Centre for Pulmonary Hypertension Royal Brompton Hospital & Imperial College London London, UK
Disclaimers
- Unrestricted educational grants from Actelion, GSK,
Pfizer
- Consultant/speaker for Actelion, Pfizer
- RBH: unrestricted research grants from Actelion
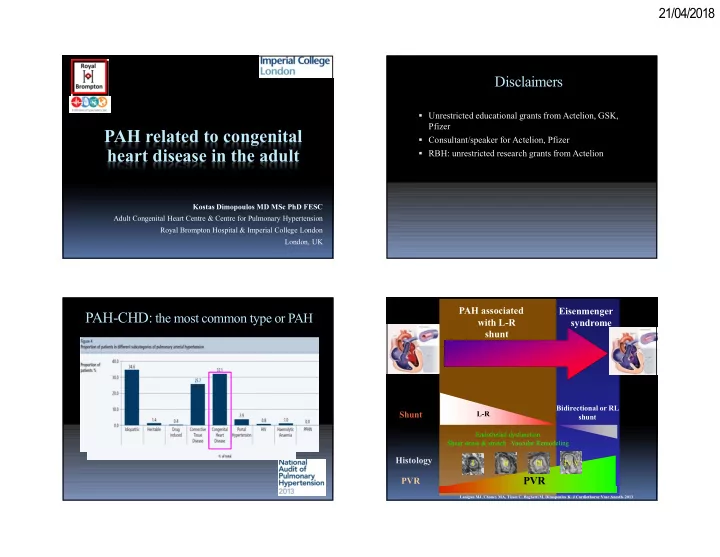
PAH-CHD: the most common type or PAH
R-L
Shunt Histology PVR
I
Shear stress & stretch Vascular Remodeling
Bidirectional or RL shunt
PAH associated with L-R shunt Eisenmenger syndrome
Endothelial dysfunction
L-R IV-V II III
PVR
Lanigan MJ, Chaney MA, Tissot C, Beghetti M, Dimopoulos K. J Cardiothorac Vasc Anesth. 2013