
SLIDE 1
1
Special stains in liver pathology
Which, why, how……Really? Sanjay Kakar, MD University of California, San Francisco Current Issues in Surgical Pathology 2014
Outline
- Which stains
- Why the stain is done
- How the stain is interpreted
Pitfalls, technical aspects
- Really
Reflex use of special stains
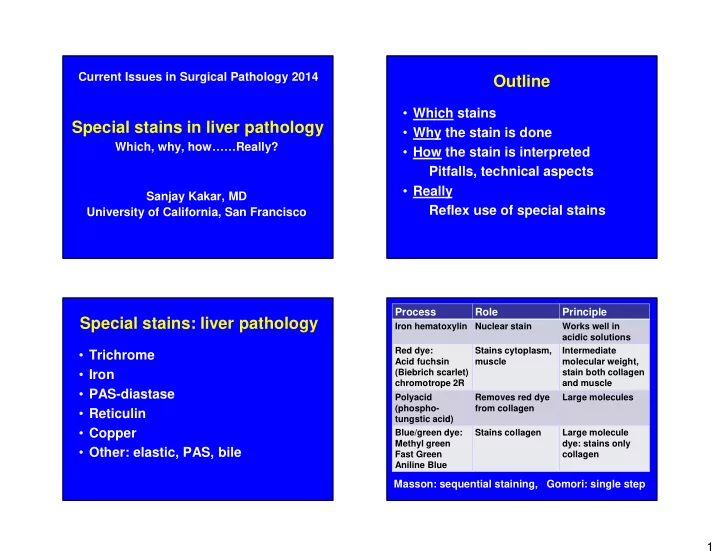
Special stains: liver pathology
- Trichrome
- Iron
- PAS-diastase
- Reticulin
- Copper
- Other: elastic, PAS, bile