
SLIDE 1
1
Bariatric Surgery: Successes and Pitfalls
Bradley J. Needleman, MD & Dara Schuster, MD The Ohio State University Columbus, OH
- Review the short term and long term
successes of bar iatric surgery
- Discuss the short term and long term
complications of bariatric surgery
- Describe the necessary medical follow-up,
monitoring and treatment plans for patients that have undergone bariatric surgery
- Recognize the need for comprehensive
weight management before and after surgery has occurred.
Objectives
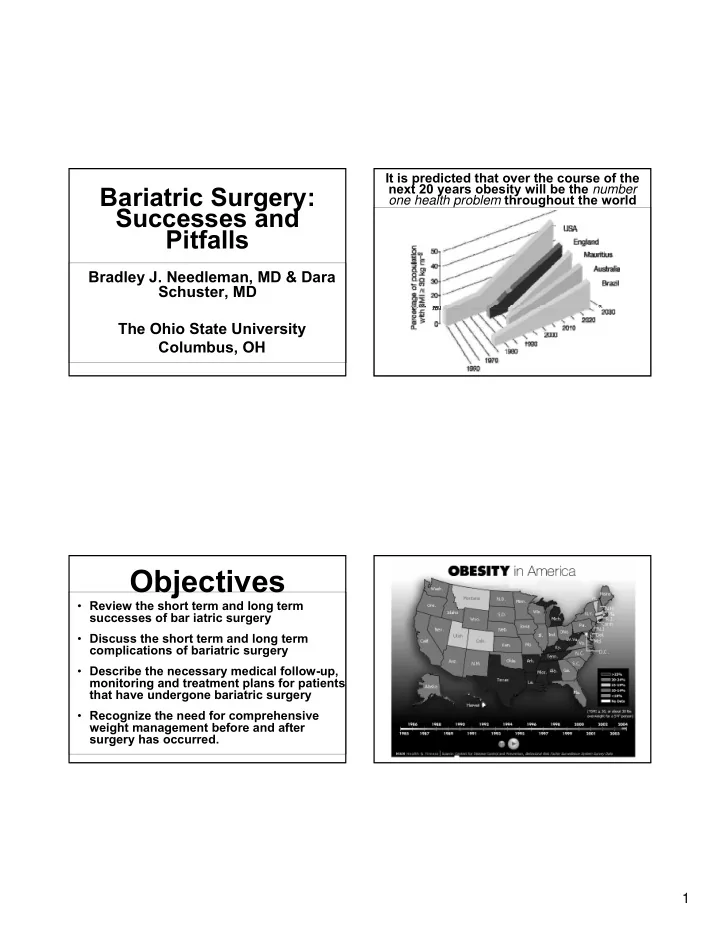
It is predicted that over the course of the next 20 years obesity will be the number
- ne health problem throughout the world